

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://www.jocmr.org |
Review
Volume 14, Number 11, November 2022, pages 441-447

Primary Recurrent Common Bile Duct Stones: Timing of Surgical Intervention
Subhi Mansoura, Yoram Klugera, b, Safi Khuria, b, c
aDepartment of General Surgery, Rambam Health Care Campus, Haifa, Israel
bHPB and Surgical Oncology Unit, Rambam Health Care Campus, Haifa, Israel
cCorresponding Author: Safi Khuri, Department of General Surgery, Rambam Health Care Campus, Haa’leya Hashniya, Haifa 31096, Israel
Manuscript submitted September 16, 2022, accepted October 24, 2022, published online November 29, 2022
Short title: Primary Recurrent CBDS
doi: https://doi.org/10.14740/jocmr4826
- Abstract
- Introduction
- Risk Factors for Recurrent CBDS
- Surgical Intervention
- Discussion
- Conclusion
- References
| Abstract | ▴Top |
Cholelithiasis (gallstones) is a very common medical problem worldwide, with 5-30% of patients demonstrating a combined condition of cholelithiasis and choledocholithiasis (common bile duct stones (CBDS)). CBDS are usually classified as primary or secondary stones. Primary CBDS are defined as stones detected 2 years or more following cholecystectomy, while secondary stones, the most common type, usually migrate from the gallbladder to the bile ducts. Recurrent CBDS are defined as stones detected 6 months or more following endoscopic retrograde cholangiopancreatography (ERCP) with complete duct clearance. Although ERCP with endoscopic sphincterotomy has emerged as the main therapeutic option for CBDS, with up to 95% bile duct clearance rate, up to 25% of said patients develop recurrent bile duct stones. Thus far, several issues related to recurrent CBDS are still unclear and questions regarding this specific pathology have no precise answers: how many trials of ERCP and endoscopic sphincterotomy should be attempted before referring the patient for surgical management? Is there an association between risk factors and early surgical intervention? Thus, currently, there is no worldwide scientific-based consensus regarding the best management of this specific group of patients. The main issue for this article is to review the relevant English literature and find out the main high risk factors for recurrent CBDS, and form a diagnostic and treatment plan, hence, identifying the subgroup of patients that will benefit from early surgical management, preventing further ERCP-associated complications.
Keywords: Recurrent CBDS; ERCP; Endoscopic sphincterotomy; Risk factors; Surgical intervention
| Introduction | ▴Top |
Gallstone disease (cholelithiasis) is a very common medical problem worldwide, especially in developed countries [1, 2]. A significant difference of cholelithiasis by ethnicity/race is noted, with Hispanic people of Central and North America having the highest prevalence rate [3]. Although most of these patients remain asymptomatic throughout their lifetimes, 10-25% suffer various gastrointestinal symptoms and develop complications [4-6]. Five to thirty percent of patients have combined cholelithiasis and choledocholithiasis (common bile duct stones (CBDS)) at the time of diagnosis [7]. CBDS are usually classified as primary, when detected 2 years or more following cholecystectomy, or as secondary, originating from the gallbladder, when detected up to 2 years following cholecystectomy. Recurrent CBDS are defined as stones found 6 months or more following initial endoscopic retrograde cholangiopancreatography (ERCP) with complete duct clearance [8, 9].
While cholesterol stones are the most common gallstones (75-80%), recurrent CBDS are usually pigment stones, mainly brown stones, associated with recurrent biliary infections [10, 11]. The hypothesis behind this association is that, following ERCP and endoscopic sphincterotomy, a laxity of the sphincter of Oddi develops, and this in turn causes backward flow of duodenal contents into the biliary and pancreatic ducts, and thus, recurrent infections with stone formation.
Recurrent CBDS could be asymptomatic, found incidentally by radiological tests made for non-relevant disease, or it could be symptomatic, presenting as obstructive jaundice, acute suppurative ascending cholangitis, pancreatitis, etc. [11].
Since its introduction in 1974, initially as a procedure of choice for elderly unfit patients for surgical management of CBDS, ERCP with endoscopic sphincterotomy has become the procedure of choice for the treatment of CBDS in all category of patients worldwide [12]. Although the procedure is usually considered safe and effective, it is not an innocuous one and complications (4-16%), either early or late, may develop. Early complications include post-ERCP pancreatitis (the most common - up to 6%), hemorrhage, cholangitis and perforation (the least common reported in 0.08-1% of cases) [13-15]. Late complications include papillary stenosis or recurrent CBDS, with the latter growing into a burden for both the patients and the healthcare systems.
Although ERCP along with endoscopic sphincterotomy is considered the first-line therapeutic modality for CBDS, several issues related to recurrent CBDS are still unclear and questions regarding this specific pathology have no clearcut answers: how many trials of ERCP and endoscopic sphincterotomy should be attempted before referring the patient for surgical management? Following which episode of symptomatic recurrent CBDS the patient should be operated on? And is there an association between risk factors and early surgical intervention?
The absence of answers for the aforementioned questions is the main reason for the absence of worldwide scientific-based therapeutic consensus regarding primary recurrent CBDS.
This review article is to find out the possible independent risk factors for primary recurrent CBDS and further determine its potential association with surgical intervention.
| Risk Factors for Recurrent CBDS | ▴Top |
Stones of the gallbladder and bile duct are usually classified into three major types: cholesterol stones, pigment stones and mixed stones [16, 17]. Cholesterol stones are the major type (75-80%) usually containing more than 50% cholesterol. Risk factors for cholesterol stone formation include hyperlipidemia, female gender, total parenteral nutrition and others. Pigment stones include black stones, associated with hemolysis and liver cirrhosis, and brown stones (the most common type of CBDS) which are associated with recurrent bile duct infection [10, 11, 18]. Pigmented stones, mainly the brown type, are the most common type of primary recurrent CBDS.
In addition to recurrent bile duct infection, specifically following ERCP and endoscopic sphincterotomy, other risk factors for recurrent CBDS were reported: patient’s age, patient’s gender, genetic mutations, stone’ number and size, stone location along the common bile duct (CBD), diameter of the bile ducts, the presence of duodenal diverticulum, previous ERCP with endoscopic sphincterotomy, metabolic factors, drugs and others.
Age
Age older than 65 years old is considered a very high independent risk factor for CBDS recurrence. In his study, Fritz et al [19] reported a recurrence rate of up to 30% following ERCP and endoscopic sphincterotomy in patients older than 65 years. Moreover, 86.4% of the CBDS recurrences were reported in the elderly group of patients (older than 65 years old) [20]. These findings were also demonstrated by Deng et al [7], when he concluded that age above 65 years old is regarded as an independent risk factor for CBDS recurrence following ERCP and endoscopic sphincterotomy.
Gender
Due to the high estrogen levels, it is well known that female patients are more susceptible to develop choledocholithiasis. On the other hand, as have been already reported by several studies [21, 22], there is no correlation between gender and risk of CBDS recurrence.
Genetic mutations
Several genetic mutations have been examined for gallbladder and bile duct stones formation, of which the ABCB4 mutation (encoding the hepatobiliary flippase) is the main genetic risk factor for stones recurrence [23]. The aforementioned genetic mutation leads to a defect in the multidrug resistance protein 3 (MDR3), which in turn causes phosphatidylcholine levels reduction, increasing the risk for stones formation.
The number and diameter of the CBDS
The number and diameter of stones present in the bile ducts have been the subject of controversy in the literature. The main hypothesis suggests that as the diameter and number of the stones is higher, the risk for CBDS recurrence is higher [7, 22]. Several theories can explain this, including loss of bile duct peristalsis due to dilation of the bile duct as a result of large stones, bacterial overgrowth and bile duct infection (which can predispose patients to pigment stone development) and more difficult endoscopic procedures, with higher probability for lithotripsy usage and higher failure rates.
In the study by Deng et al [7], a stone diameter of 10 mm or more was an independent risk factor for stone recurrence. The findings of Deng et al were also demonstrated in another study [22], where the recurrence rates at 5, 10 and 15 years were higher when stone diameter was 11 mm or more. These findings were contradicted by several studies that concluded there is no correlation between stone size and risk of CBDS recurrence [24, 25].
Several studies demonstrated that multiple bile duct stones (two or more) is a risk factor for CBDS recurrence with proven statistical significance [26, 27]. Although patients with multiple bile duct stones had a higher rate of recurrence, it was not significant statistically in relation to the control group in the study by Deng et al [7]. Larger number and size of stones could be a risk for residual bile duct stones rather than risk for recurrence as reported by Cheon and Lehman [24], and thus, the outcomes are related more to management methods than patient factors.
Stone position
Stone position along the CBD was mentioned as a possible risk factor for recurrence. It was suggested that as the stone is more distally located and close to the sphincter of Oddi, the greater the pressure it causes with massive damage [28]. Up till now, there is no currently published study regarding this issue, and future studies are encouraged to investigate this suggestion.
CBD diameter
The diameter of the CBD as a risk factor for CBDS recurrence was examined extensively during the last two decades and most studies report a strong correlation. The hypothesis behind this correlation is that dilation of the bile duct causes functional impairment of bile duct peristalsis, which in turn leads to stasis, bacterial infection and stone formation [29]. In his study, Pereira-Lima et al [30] showed that the risk for CBDS recurrence was four-folds higher in patients with CBD diameter of 15 mm or higher than in patients with CBD diameter of 10 mm or less. The risk of CBDS recurrence was 46% in patients with CBD diameter of more than 15 mm compared to only 20% in patients with CBD diameter of less than 12 mm [31]. A common bile duct of more than 15 mm was also a strong risk factor for CBDS recurrence with statistical significance in the study by Li et al [27]. The finding of strong correlation between CBD diameter and CBDS recurrence was also demonstrated in several other studies [7, 26, 32, 33]. Although the diameter of the CBD is already a confirmed strong risk factor for CBDS recurrence, the precise diameter is yet to be known, as different diameters had shown different recurrence rates. A consensus is that a CBD diameter of 15 mm or more is a high risk factor for recurrent CBDS.
Periampullary diverticulum
The presence of duodenal periampullary diverticulum had also been reported as a risk factor for CBDS recurrence. Duodenal diverticulum, firstly recognized in 1710 by Chomel, is uncommon with an incidence rate of 15-22% by post mortem studies [34, 35]. Periampullary diverticula is the most common type of duodenal diverticulum, usually located within 2 - 3 cm from the papilla of Vater [36]. Three different types of periampullary diverticulum are known, depending on the location of the major papilla: type A - inside the diverticulum, type B - adjacent to the diverticulum and type C - outside the diverticulum. Although the precise mechanism is yet to be known, it is already proved that periampullary diverticulum is a strong predisposing factor for stone formation as well as stone recurrence [37, 38]. The most accepted mechanism according to manometric studies is that the presence of periampullary diverticulum leads to decreased pressure in the sphincter of Oddi, which in turn leads to backflow of intestinal flora to the bile duct and the formation of pigment stones. The reported incidence of bile duct stones (mainly pigment stones) in patients with periampullary diverticulum is almost 89% [39].
ERCP
Although ERCP, especially when accompanied by endoscopic sphincterotomy, is the main therapeutic option for CBDS, it is regarded as a risk factor for CBDS recurrence. Following endoscopic sphincterotomy, stricture of the papilla may develop, in addition of bile duct dilation and infection. These in turn may cause CBDS recurrence. In his study which included 11 centers, Yasuda et al [40] demonstrate that ERCP with endoscopic sphincterotomy is an independent risk factor for CBDS recurrence. CBDS recurrence can develop following either ERCP with endoscopic sphincterotomy, balloon dilatation or stent insertion. The risk of recurrence was less after balloon dilatation (8.5%) than endoscopic sphincterotomy (15%) on follow-up period of more than 90 months [41]. Similar findings were also reported in the study by Kojima et al [42]. Following balloon dilatation, the function of the sphincter of Oddi was preserved in 70% of patients. ERCP with either endoscopic sphincterotomy, balloon dilatation or stent insertion was regarded as an independent risk factor for CBDS recurrence [7, 22], with endoscopic sphincterotomy patients having the higher rates of recurrences. Biliary stent insertion is considered an alternative option mainly for unstable patients, due to severe ascending cholangitis, and for elderly patients. Interesting findings were reported by Choi et al [43]; in his study which included 483 patients, Choi et al showed that patients who have had stent insertions to the bile duct for a short period had less risk for recurrent CBDS. On the other hand, stent insertion for a long time was an independent risk factor for CBDS recurrence [44].
Other factors
Metabolic related risk factors for gallbladder and bile duct stones are diverse and include: obesity, hyperlipidemia, insulin resistance diabetes mellitus, fatty liver, hypercalcemia and hyperuricemia [45]. Although there is no study investigating the correlation between these factors and primary CBDS recurrence, it is believed that these should be regarded as risk factors for recurrence.
Of the several drugs investigated, proton pump inhibitors (PPIs) were found to increase the risk for CBDS recurrence, especially following ERCP and endoscopic sphincterotomy [46]. PPIs cause duodenal flora changes with bacterial overgrowth and recurrent ascending cholangitis.
| Surgical Intervention | ▴Top |
Surgical managements of CBDS have decreased dramatically since the introduction of ERCP as the main therapeutic procedure [12]. Nowadays, the role and timing of surgical intervention, especially for recurrent CBDS, is unknown due to lack of studies (mainly prospective) that compare it with other therapeutic procedures. It is usually indicated in very special cases as failure or unavailability of endoscopic management and other procedures such as percutaneous transhepatic biliary drainage (PTBD). Surgical procedures usually include CBD exploration, either by open or minimally invasive (laparoscopy) techniques, along with choledochoscopy, intra-operative cholangiogram, stone extraction with T-tube insertion, choledocho-duodenostomy/jejunostomy or resection of CBD with Roux-en-Y gastrointestinal reconstruction [47]. Due to technological advancement, laparoscopic bile duct exploration has become very safe and cost-effective [48, 49]. Stone clearance rate is up to 95% following laparoscopic CBD exploration, with morbidity and mortality rates of 4-16% and 0-2%, respectively [50, 51]. In the study by Tai et al [52], stone clearance rate was 100%, with 0% recurrence rate on a median follow-up of 16 months. Patients treated by this approach have a shorter hospital stay and lower hospital costs than patients treated by ERCP and endoscopic sphincterotomy [49]. Variable lithotripsy maneuvers, such as laser, electrohydraulic and extracorporeal shockwave, have been described with different results. These therapeutic options are barely used nowadays due to its high risk of bile duct wall damage and bleeding [53].
CBD exploration by an open approach is another accepted surgical therapeutic option, with high clearance rates of bile duct stones. In his meta-analysis, Martin et al [54] demonstrated higher rates of successful stone clearance than ERCP, with no morbidity and mortality difference. On the other hand, bile duct stone clearance rates were identical for laparoscopic bile duct exploration and ERCP, with identical morbidity and mortality rates. In another study, the recurrence rate for primary CBDS following ERCP with endoscopic sphincterotomy was higher (46%) than for open surgical exploration of the bile ducts with lithotripsy alone (29%) and open surgical bile duct exploration with lithotripsy and choledochojejunostomy (3%) [55]. There was no significant difference in complication rates for the previously mentioned therapeutic options.
Open surgical exploration of the bile ducts can be approached either by choledocho-enterostomy, stone extraction with T-tube insertion or by sphincterotomy [56]. Choledocho-enterostomy is the preferred option in the presence of multiple stones and when bile ducts are dilated more than 2 cm. This can be contemplated by resection of the bile ducts with Roux-en-Y choledochojejunostomy or with choledocho-duodenostomy without resection. One of the main complications of the latter procedure is “sump syndrome”, which develops in 1% of patients, when food or debris stagnates in the distal part of the CBD distal to the anastomosis [56].
Both surgical options, the laparoscopic and the open approach, are an accepted surgical procedure and depend mainly on the surgeon’s experience, which should dictate which option to perform.
| Discussion | ▴Top |
Since its introduction during the early 1970s, ERCP with endoscopic sphincterotomy has gained a worldwide acceptance as the main therapeutic option for CBDS. Although this non-surgical procedure is regarded as safe and highly successful, complications, either early or late, mild or severe, may develop. Of the late complications, recurrent primary CBDS is well known, and has emerged as a main topic of investigation during the last two decades due to its heavy burden on health institutions. Recurrent primary CBDS could be asymptomatic and discovered incidentally, or symptomatic with variable presentations, such as obstructive jaundice, ascending suppurative cholangitis or biliary pancreatitis.
Although risk factors for recurrent primary CBDS have been studied in a very thorough manner by previous already published retrospective studies and review articles, no manuscript discussed the correlation between these risk factors and therapeutic strategies to be followed by the treating physicians. Hence, the number of ERCP trials to be performed for the management of recurrent primary CBDS is unknown, making treatment of this unique group of patients physician-based and not scientific-based.
As mentioned before, several risk factors have strong association with CBDS recurrence with statistical significance. These factors, which include age older than 65 years old, specific genetic mutations (mainly ABCB4 mutation), dilated CBD (more than 15 mm), periampullary duodenal diverticulum and previous ERCP with endoscopic sphincterotomy should be regarded as high risk factors for stones recurrence (Table 1).
 Click to view | Table 1. Level of Risk for the Relevant Risk Factors for Recurrent CBDS |
Literature controversy exists for other reported risk factors, mainly stone diameter and number and ERCP with balloon dilatation or stent insertion. As have been mentioned earlier, variable outcomes in terms of level of risk have been shown and failure of these factors to meet statistical significance in all published articles. Therefore, multiple CBDS (more than one), large diameter of the stone (more than 1 cm) and ERCP with balloon dilatation or stent insertion may be regarded as intermediate risk factors for recurrent primary CBDS.
In the absence of scientific evidence for a strict correlation, known risk factors for stone formation such as metabolic related factors, female gender, drugs (mainly PPI) and stone position along the biliary tree, may be regarded as a low risk for recurrence.
Nowadays, it is well known that the risk for recurrence of CBDS is directly proportional to the number of recurrences. As the number increases, the risk increases as well. In his study which included 46,181 patients, Park et al [57] showed first, second and third recurrence rates of 11.3%, 23.4% and 33.4%, respectively on a median follow-up of 4.2 years. High rates of 19.5% for second recurrence and 44% for third recurrence were also reported [6]. Recurrent endoscopic intervention may cause recurrent sphincter of Oddi and bile duct epithelial injury, leading to inflammation, necrosis, scar formation and stenosis. This in turn will increase the risk for CBDS recurrence.
Due to the aforementioned histological changes and risk for bile duct stenosis and CBDS recurrence, patients with recurrent primary CBDS should be managed by a multidisciplinary team of physicians consisting of hepatobiliary surgeons, interventional gastroenterologists and abdominal radiologists.
A suggested therapeutic flow chart is shown in Figure 1.
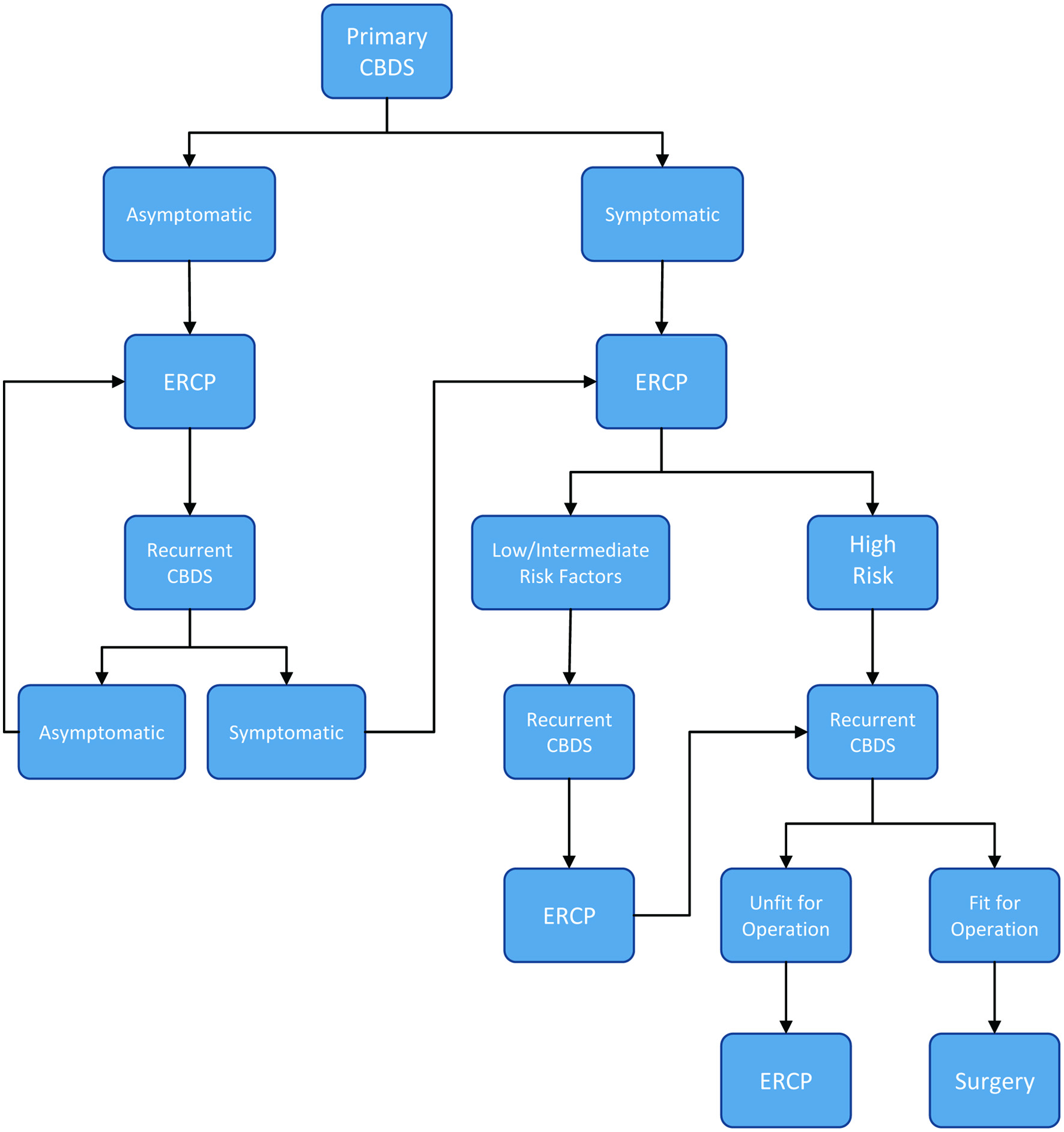 Click for large image | Figure 1. A suggested flow chart for the management of recurrent primary CBDS according to risk factors. CBDS: common bile duct stone. |
Primary recurrent CBDS may be classified into two major groups: asymptomatic and symptomatic. ERCP should be the initial therapeutic procedure for both. Of the symptomatic group, patients with one or more high risk factors should be identified during the first episode and labelled as high risk group for recurrence. This group should be considered for early surgical management, if a second symptomatic episode occurs and the patient is fit for surgical intervention. Patients who are at high risk for operation should be scheduled for repeated ERCP. Symptomatic patients with intermediate or low risk factors should be treated by a repeated ERCP if a second episode develops, and planned for surgical intervention if a third symptomatic episode occurs. Following initial management by ERCP for asymptomatic patients, a repeated ERCP should follow if patients develop recurrence accompanied by symptoms. If future recurrences develop, continuation of management will be identical to the symptomatic group.
| Conclusion | ▴Top |
Primary recurrent CBDS are uncommon, yet a known late complication of ERCP procedures and pose a heavy burden on health systems. Risk factors are well known, but their effect on therapeutic decisions has never been tested. In the absence of therapeutic consensus, a multidisciplinary team management approach is highly recommended, and patients with high risk factors should be identified and referred for early surgical intervention if a second symptomatic episode develops.
Acknowledgments
None to declare.
Financial Disclosure
This is a self-financed manuscript without funding source.
Conflict of Interest
None to declare.
Author Contributions
SM collected and analyzed the data. SK contributed to writing the manuscript. The paper was drafted by SM and SK. Critical revisions and final approval were made by YK and SK.
Data Availability
The authors declare that data supporting the findings of this study are available within the article.
| References | ▴Top |
- Everhart JE, Khare M, Hill M, Maurer KR. Prevalence and ethnic differences in gallbladder disease in the United States. Gastroenterology. 1999;117(3):632-639.
doi - Shaffer EA. Gallstone disease: Epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol. 2006;20(6):981-996.
doi pubmed - Figueiredo JC, Haiman C, Porcel J, Buxbaum J, Stram D, Tambe N, Cozen W, et al. Sex and ethnic/racial-specific risk factors for gallbladder disease. BMC Gastroenterol. 2017;17(1):153.
doi pubmed - Barbara L, Sama C, Morselli Labate AM, Taroni F, Rusticali AG, Festi D, Sapio C, et al. A population study on the prevalence of gallstone disease: the Sirmione Study. Hepatology. 1987;7(5):913-917.
doi pubmed - Fein M, Bueter M, Sailer M, Fuchs KH. Effect of cholecystectomy on gastric and esophageal bile reflux in patients with upper gastrointestinal symptoms. Dig Dis Sci. 2008;53(5):1186-1191.
doi pubmed - Gracie WA, Ransohoff DF. The natural history of silent gallstones: the innocent gallstone is not a myth. N Engl J Med. 1982;307(13):798-800.
doi pubmed - Deng F, Zhou M, Liu PP, Hong JB, Li GH, Zhou XJ, Chen YX. Causes associated with recurrent choledocholithiasis following therapeutic endoscopic retrograde cholangiopancreatography: A large sample sized retrospective study. World J Clin Cases. 2019;7(9):1028-1037.
doi pubmed - Tanaka M, Ikeda S, Yoshimoto H, Matsumoto S. The long-term fate of the gallbladder after endoscopic sphincterotomy. Complete follow-up study of 122 patients. Am J Surg. 1987;154(5):505-509.
doi - Bergman JJ, van der Mey S, Rauws EA, Tijssen JG, Gouma DJ, Tytgat GN, Huibregtse K. Long-term follow-up after endoscopic sphincterotomy for bile duct stones in patients younger than 60 years of age. Gastrointest Endosc. 1996;44(6):643-649.
doi - Leuschner U, Guldutuna S, Hellstern A. Etiology, pathogenesis and therapy of pigment gallstones. Dig Dis. 1991;9(5):282-293.
doi pubmed - Ostrow JD. The etiology of pigment gallstones. Hepatology. 1984;4(5 Suppl):215S-222S.
doi pubmed - Kawai K, Akasaka Y, Murakami K, Tada M, Koli Y. Endoscopic sphincterotomy of the ampulla of Vater. Gastrointest Endosc. 1974;20(4):148-151.
doi - Freeman ML. Adverse outcomes of endoscopic retrograde cholangiopancreatography: avoidance and management. Gastrointest Endosc Clin N Am. 2003;13(4):775-798.
doi - Lai CH, Lau WY. Management of endoscopic retrograde cholangiopancreatography-related perforation. Surgeon. 2008;6(1):45-48.
doi - Cotton PB, Garrow DA, Gallagher J, Romagnuolo J. Risk factors for complications after ERCP: a multivariate analysis of 11,497 procedures over 12 years. Gastrointest Endosc. 2009;70(1):80-88.
doi pubmed - Saharia PC, Zuidema GD, Cameron JL. Primary common duct stones. Ann Surg. 1977;185:598-604.
doi pubmed - Cariati A. Gallstone classification in Western countries. Indian J Surg. 2015;77(Suppl 2):376-380.
doi pubmed - Soloway RD, Trotman BW, Ostrow JD. Pigment gallstones. Gastroenterology. 1977;72(1):167-182.
doi - Fritz E, Kirchgatterer A, Hubner D, Aschl G, Hinterreiter M, Stadler B, Knoflach P. ERCP is safe and effective in patients 80 years of age and older compared with younger patients. Gastrointest Endosc. 2006;64(6):899-905.
doi pubmed - Parra-Membrives P, Martinez-Baena D, Lorente-Herce JM, Jimenez-Riera G, Sanchez-Galvez MA. Choledocholithiasis recurrence following laparoscopic common bile duct exploration. Cir Esp (Engl Ed). 2019;97(6):336-342.
doi pubmed - Kim DI, Kim MH, Lee SK, Seo DW, Choi WB, Lee SS, Park HJ, et al. Risk factors for recurrence of primary bile duct stones after endoscopic biliary sphincterotomy. Gastrointest Endosc. 2001;54(1):42-48.
doi pubmed - Ando T, Tsuyuguchi T, Okugawa T, Saito M, Ishihara T, Yamaguchi T, Saisho H. Risk factors for recurrent bile duct stones after endoscopic papillotomy. Gut. 2003;52(1):116-121.
doi pubmed - Rosmorduc O, Hermelin B, Boelle PY, Parc R, Taboury J, Poupon R. ABCB4 gene mutation-associated cholelithiasis in adults. Gastroenterology. 2003;125(2):452-459.
doi - Cheon YK, Lehman GA. Identification of risk factors for stone recurrence after endoscopic treatment of bile duct stones. Eur J Gastroenterol Hepatol. 2006;18(5):461-464.
doi pubmed - Lujian P, Xianneng C, Lei Z. Risk factors of stone recurrence after endoscopic retrograde cholangiopancreatography for common bile duct stones. Medicine (Baltimore). 2020;99(27):e20412.
doi pubmed - Yoo ES, Yoo BM, Kim JH, Hwang JC, Yang MJ, Lee KM, Kim SS, et al. Evaluation of risk factors for recurrent primary common bile duct stone in patients with cholecystectomy. Scand J Gastroenterol. 2018;53(4):466-470.
doi pubmed - Li S, Su B, Chen P, Hao J. Risk factors for recurrence of common bile duct stones after endoscopic biliary sphincterotomy. J Int Med Res. 2018;46(7):2595-2605.
doi pubmed - Wu Y, Xu CJ, Xu SF. Advances in risk factors for recurrence of common bile duct stones. Int J Med Sci. 2021;18(4):1067-1074.
doi pubmed - Ueno N, Ozawa Y, Aizawa T. Prognostic factors for recurrence of bile duct stones after endoscopic treatment by sphincter dilation. Gastrointest Endosc. 2003;58(3):336-340.
doi - Pereira-Lima JC, Jakobs R, Winter UH, Benz C, Martin WR, Adamek HE, Riemann JF. Long-term results (7 to 10 years) of endoscopic papillotomy for choledocholithiasis. Multivariate analysis of prognostic factors for the recurrence of biliary symptoms. Gastrointest Endosc. 1998;48(5):457-464.
doi - Nzenza TC, Al-Habbal Y, Guerra GR, Manolas S, Yong T, McQuillan T. Recurrent common bile duct stones as a late complication of endoscopic sphincterotomy. BMC Gastroenterol. 2018;18(1):39.
doi pubmed - Park SY, Hong TH, Lee SK, Park IY, Kim TH, Kim SG. Recurrence of common bile duct stones following laparoscopic common bile duct exploration: a multicenter study. J Hepatobiliary Pancreat Sci. 2019;26(12):578-582.
doi pubmed - Song ME, Chung MJ, Lee DJ, Oh TG, Park JY, Bang S, Park SW, et al. Cholecystectomy for prevention of recurrence after endoscopic clearance of bile duct stones in Korea. Yonsei Med J. 2016;57(1):132-137.
doi pubmed - Christoforidis E, Goulimaris I, Kanellos I, Tsalis K, Dadoukis I. The role of juxtapapillary duodenal diverticula in biliary stone disease. Gastrointest Endosc. 2002;55(4):543-547.
doi pubmed - Kim CW, Chang JH, Kim JH, Kim TH, Lee IS, Han SW. Size and type of periampullary duodenal diverticula are associated with bile duct diameter and recurrence of bile duct stones. J Gastroenterol Hepatol. 2013;28(5):893-898.
doi pubmed - Lobo DN, Balfour TW, Iftikhar SY, Rowlands BJ. Periampullary diverticula and pancreaticobiliary disease. Br J Surg. 1999;86(5):588-597.
doi pubmed - Li X, Zhu K, Zhang L, Meng W, Zhou W, Zhu X, Li B. Periampullary diverticulum may be an important factor for the occurrence and recurrence of bile duct stones. World J Surg. 2012;36(11):2666-2669.
doi pubmed - Kato S, Chinen K, Shinoura S, Kikuchi K. Predictors for bile duct stone recurrence after endoscopic extraction for naive major duodenal papilla: A cohort study. PLoS One. 2017;12(7):e0180536.
doi pubmed - Zhou B, Hu J, Zhong Y. Surgical treatments for patients with recurrent bile duct stones and Oddis sphincter laxity. Intractable Rare Dis Res. 2017;6(3):172-176.
doi pubmed - Yasuda I, Fujita N, Maguchi H, Hasebe O, Igarashi Y, Murakami A, Mukai H, et al. Long-term outcomes after endoscopic sphincterotomy versus endoscopic papillary balloon dilation for bile duct stones. Gastrointest Endosc. 2010;72(6):1185-1191.
doi pubmed - Doi S, Yasuda I, Mukai T, Iwashita T, Uemura S, Yamauchi T, Nakashima M, et al. Comparison of long-term outcomes after endoscopic sphincterotomy versus endoscopic papillary balloon dilation: a propensity score-based cohort analysis. J Gastroenterol. 2013;48(9):1090-1096.
doi pubmed - Kojima Y, Nakagawa H, Miyata A, Hirai T, Ohyama I, Okada A, Hiramatsu T, et al. Long-term prognosis of bile duct stones: endoscopic papillary balloon dilatation versus endoscopic sphincterotomy. Dig Endosc. 2010;22(1):21-24.
doi pubmed - Choi JH, Lee TY, Cheon YK. Effect of stent placement on stone recurrence and post-procedural cholangitis after endoscopic removal of common bile duct stones. Korean J Intern Med. 2021;36(Suppl 1):S27-S34.
doi pubmed - Kaneko J, Kawata K, Watanabe S, Chida T, Matsushita M, Suda T, Kobayashi Y. Clinical characteristics and risk factors for stent-stone complex formation following biliary plastic stent placement in patients with common bile duct stones. J Hepatobiliary Pancreat Sci. 2018;25(10):448-454.
doi pubmed - Lammert F, Gurusamy K, Ko CW, Miquel JF, Mendez-Sanchez N, Portincasa P, van Erpecum KJ, et al. Gallstones. Nat Rev Dis Primers. 2016;2:16024.
doi pubmed - Fukuba N, Ishihara S, Sonoyama H, Yamashita N, Aimi M, Mishima Y, Mishiro T, et al. Proton pump inhibitor is a risk factor for recurrence of common bile duct stones after endoscopic sphincterotomy - propensity score matching analysis. Endosc Int Open. 2017;5(4):E291-E296.
doi pubmed - Cai JS, Qiang S, Bao-Bing Y. Advances of recurrent risk factors and management of choledocholithiasis. Scand J Gastroenterol. 2017;52(1):34-43.
doi pubmed - Clayton ES, Connor S, Alexakis N, Leandros E. Meta-analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. Br J Surg. 2006;93(10):1185-1191.
doi pubmed - Poulose BK, Arbogast PG, Holzman MD. National analysis of in-hospital resource utilization in choledocholithiasis management using propensity scores. Surg Endosc. 2006;20(2):186-190.
doi pubmed - Rojas-Ortega S, Arizpe-Bravo D, Marin Lopez ER, Cesin-Sanchez R, Roman GR, Gomez C. Transcystic common bile duct exploration in the management of patients with choledocholithiasis. J Gastrointest Surg. 2003;7(4):492-496.
doi - Thompson MH, Tranter SE. All-comers policy for laparoscopic exploration of the common bile duct. Br J Surg. 2002;89(12):1608-1612.
doi pubmed - Tai CK, Tang CN, Ha JP, Chau CH, Siu WT, Li MK. Laparoscopic exploration of common bile duct in difficult choledocholithiasis. Surg Endosc. 2004;18(6):910-914.
doi pubmed - Evans JA, Branch MS. The recalcitrant bile duct stone. Tech Gastrointest Endosc. 2007;9(2)104-113.
doi - Martin DJ, Vernon DR, Toouli J. Surgical versus endoscopic treatment of bile duct stones. Cochrane Database Syst Rev. 2006;2:CD003327.
doi - Xia H, Xin X, Zhang H, et al. Causes and surgical management of choledocholithiasis after cholecystectomy. Research Square. 2022.
doi - Baker AR, Neoptolemos JP, Leese T, James DC, Fossard DP. Long term follow-up of patients with side to side choledochoduodenostomy and transduodenal sphincteroplasty. Ann R Coll Surg Engl. 1987;69(6):253-257.
- Park BK, Seo JH, Jeon HH, Choi JW, Won SY, Cho YS, Lee CK, et al. A nationwide population-based study of common bile duct stone recurrence after endoscopic stone removal in Korea. J Gastroenterol. 2018;53(5):670-678.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.