

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 7, Number 7, July 2015, pages 560-563
Retreatment of a Maxillary Lateral Incisor With Two Separate Root Canals Confirmed With Cone Beam Computed Tomography
Seda Aydemira, Dilek Helvacioglu-Yigita, Alper Sinanoglub, Emre Ozelc, d
aDepartment of Endodontics, Faculty of Dentistry, University of Kocaeli, Kocaeli, Turkey
bDepartment of Oral and Maxillofacial Radiology, Faculty of Dentistry, University of Kocaeli, Kocaeli, Turkey
cDepartment of Restorative Dentistry, Faculty of Dentistry, University of Kocaeli, Kocaeli, Turkey
dCorresponding Author: Emre Ozel, Department of Restorative Dentistry, Faculty of Dentistry, University of Kocaeli, Yuvacik, Basiskele, Kocaeli, Turkey
Manuscript accepted for publication April 02, 2015
Short title: Maxillary Lateral Incisor With Two Root Canals
doi: http://dx.doi.org/10.14740/jocmr2154w
| Abstract | ▴Top |
The purpose of this report is to present a rare case of a maxillary lateral incisor exhibiting two separate root canals confirmed by cone-beam computed tomography (CBCT). A 65-year-old female patient with an esthetic complaint regarding her maxillary left lateral incisor was referred to our clinic. During a radiographical examination, an endodontically treated root canal and an extra root canal with an apical lesion were observed. The retreatment was performed. CBCT findings confirmed the root canal mophology of the maxillary left lateral with two distinct canals. We conclude that the CBCT imaging is an adjunctive tool for better assessment of complex root canal systems.
Keywords: Cone-beam computed tomography; Endodontic retreatment; Extra root canal; Maxillary lateral incisor
| Introduction | ▴Top |
It is well known that the success of endodontic therapy depends on the complete cleaning and shaping of the root canal systems, three-dimensional obturation, and proper coronary sealing. To obtain successful root canal treatment, knowledge of the morphology of the root canal system as well as its variations is essential. The maxillary left lateral incisor is known to display anatomical variations.
The two-canal morphology of the mandibular premolars is rarely considered in diagnostic radiography. The separation of the secondary canal with an acute angle means the second canal remains undiagnosed both by radiography and tactile examination [1]. Undetected canals are the cause of 42% of root canal retreatments [2]. Cone-beam computed tomography (CBCT) is a non-invasive technique to determine the existence of an extra root canal. It reveals the true nature of macrostructure three-dimensionally and its curvature and angulation [3]. CBCT presents the precise position of the extra root canal; hence, it helps to track the curvature and prevents iatrogenic errors that might occur in relation to canal curvature such as instrument separation, perforation, and ledge formation.
The purpose of this report is to present a rare case of maxillary lateral incisor exhibiting two separate root canals that was confirmed by CBCT findings.
| Case Report | ▴Top |
A 65-year-old female patient with an esthetic complaint regarding her maxillary left lateral incisor was referred to our clinic. During a radiographic examination, an endodontically treated root canal and an extra root canal with an apical lesion were observed (Fig. 1). The existing root filling was removed using ProTaper Universal retreatment files (Dentsply Maillefer, Ballaigues, Switzerland). D1, D2 and D3 retreatment files were used in the crown-down technique with a low torque motor (VDW Silver; VDW). The missing root canal was located and the working length of both root canals was measured with an apex locator Raypex 6 (VDW, Munich, Germany) and confirmed with a periapical radiograph (Fig. 2).
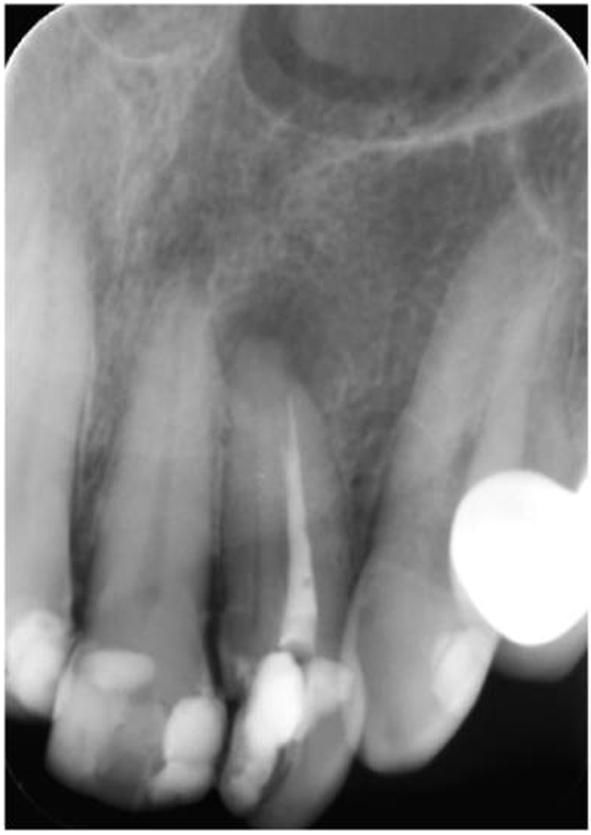 Click for large image | Figure 1. Preoperative periapical radiography. |
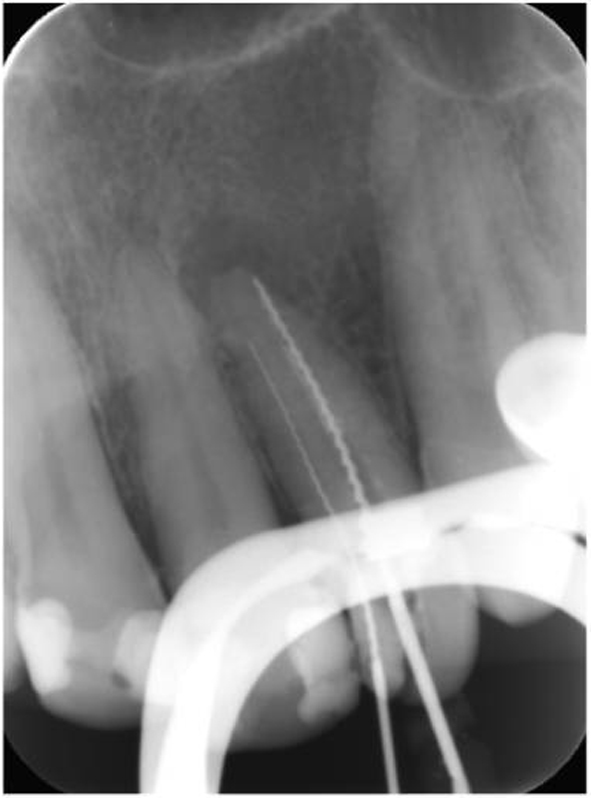 Click for large image | Figure 2. Working length determination. |
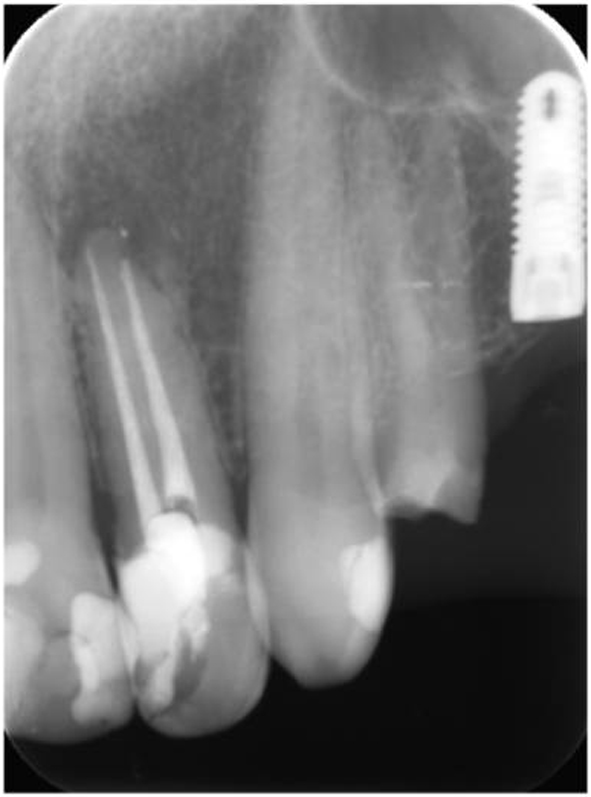
The root canals were then shaped with ProTaper Universal instruments (Dentsply Maillefer, Ballaigues, Switzerland) with a sequence of SX, S1, S2, F1 and F2 according to the manufacturer’s instructions. The root canals were lubricated with MM-EDTA cream (Micro-Mega, Besancon, France), and irrigated with 2 mL of 2.5% NaOCl between instruments and then obturated using cold lateral compaction of gutta-percha (Diadent, Seoul, South Korea) with AH Plus sealer (Dentsply De Trey GmbH, Konstanz, Germany) (Fig. 3).
 Click for large image | Figure 3. Postoperative periapical radiography. |
The patient was also referred to the Department of Oral and Maxillofacial Radiology for CBCT evaluation of her maxilla for implant site assessment (Planmeca ProMax 3D Max, Planmeca Oy, Helsinki, Finland). Axial, panoramic and cross-sectional images were reconstructed with a slice thickness of 1 mm. CBCT findings confirmed the root canal morphology of the maxillary left lateral with two separate canals.
Following the root canal treatment, the tooth was etched with 37% phosphoric acid, and restored with an adhesive system (Single Bond Universal Adhesive, 3M ESPE, USA) and nanocomposite (Filtek Ultimate Universal Restorative, 3M ESPE, USA). Finishing and polishing procedures were performed by discs and burs. A recall was carried out at the end of 18 months (Fig. 4).
 Click for large image | Figure 4. Periapical radiography after 18 months follow-up. |
During the recall, composite restoration was found successful according to the criteria of the United States Public Health Service (USPHS) (Table 1) in terms of retention, color match, secondary caries, anatomic form, marginal adaptation and surface texture (Fig. 5).
 Click to view | Table 1. United States Public Health Service (USPHS) Criteria |
 Click for large image | Figure 5. Clinical view after 18 months follow-up. |
| Discussion | ▴Top |
This report describes a rare case of a maxillary lateral incisor tooth that had two separate root canals in one root yet did not exhibit any morphological anomaly of the crown. A maxillary lateral incisor tooth most frequently exhibits a single root with a single canal [4]. However, there are a few case reports describing maxillary lateral incisor teeth with two canals [5-7], three canals [8, 9], and even four canals [10]. Many of these cases omanifest clinically as gemination, fusion, concrescence, or dens invaginatus since maxillary lateral incisors are often located at the site of high embryological risk [11-13]. In the present case, none of these abnormalities (i.e., gemination, fusion, concrescence, or dens invaginatus) was observed.
The probable etiology for unilateral accessory roots is traumatic injury of primary teeth. Root duplication may occur following intrusive luxation of primary teeth, resulting in a traumatic division of the cervical loop and thus formation of two separate roots. In these cases, a mesial and a distal root can be detected on the radiograph [14].
An emerging technology, CBCT has the ability to assess an area of interest in three dimensions, thereby eliminating the superimposition problem of conventional radiographic imaging. CBCT provides detailed and three-dimensional information concerning extra canals, apical deltas, and canal type. It provides accurate measurement potential in all aspects of root canal system, and in brief, a three-dimensional perspective of root canal anatomy [15, 16]. But use of CBCT must be limited. It may be justified for selected cases, such as when intraoral radiographs provide equivocal information on root canal anatomy or the information is inadequate for planning treatment, as is the case with multi-rooted teeth.
In the present case, the CBCT scan was not performed for endodontic purposes. The CBCT findings confirmed two separate canals in the maxillary left lateral (Fig. 6). Eighteen months after the procedure, the radiographical examination showed a decrease in the size of the periapical lesion. In addition, the composite restoration scored alpha for all USPHS criteria during the 18-month recall. The follow-up demonstrated a clinically asymptomatic and adequately functional tooth.
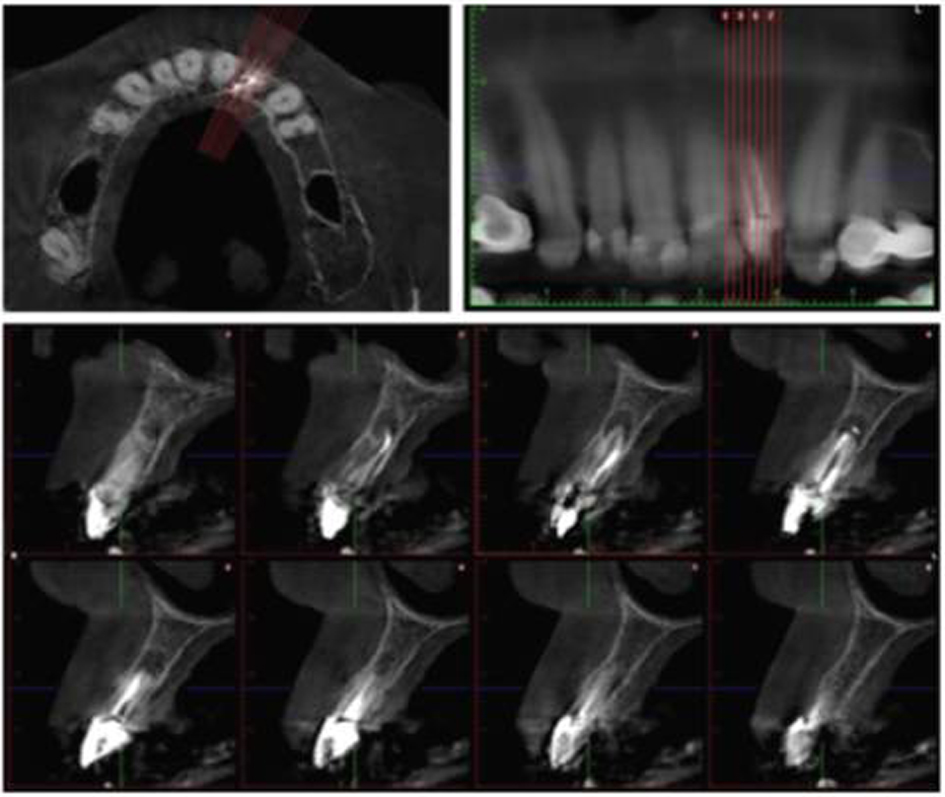 Click for large image | Figure 6. Axial, panoramic and cross-sectional reconstruction with a slice thickness at 1 mm. |
The clinician should be aware of such abnormalities in root morphology. CBCT imaging is an adjunctive tool for better assessment of complex root canal systems.
Conflict of Interest
No conflict of interest relevant to this article was reported.
| References | ▴Top |
- Yoshioka T, Villegas JC, Kobayashi C, Suda H. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod. 2004;30(2):73-74.
doi pubmed - Nallapati S. Three canal mandibular first and second premolars: a treatment approach. J Endod. 2005;31(6):474-476.
doi pubmed - Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33(9):1121-1132.
doi pubmed - Burns RC, Herbranson EJ. Tooth morphology and access cavity preparation. In: St. Louis MO. Pathways of the Pulp, 8th ed. USA: Mosby Elsevier; 2002. p. 173-229.
- Christie WH, Peikoff MD, Acheson DW. Endodontic treatment of two maxillary lateral incisors with anomalous root formation. J Endod. 1981;7(11):528-534.
doi - Friedman S, Mor H, Stabholz A. Endodontic therapy of a fused permanent maxillary lateral incisor. J Endod. 1984;10(9):449-451.
doi - Thompson BH, Portell FR, Hartwell GR. Two root canals in a maxillary lateral incisor. J Endod. 1985;11(8):353-355.
doi - Peix-Sanchez M, Minana-Laliga R. A case of unusual anatomy: a maxillary lateral incisor with three canals. Int Endod J. 1999;32(3):236-240.
doi pubmed - Jung M. Endodontic treatment of dens invaginatus type III with three root canals and open apical foramen. Int Endod J. 2004;37(3):205-213.
doi pubmed - Kottoor J, Murugesan R, Albuquerque DV. A maxillary lateral incisor with four root canals. Int Endod J. 2012;45(4):393-397.
doi pubmed - Indra R, Srinivasan MR, Farzana H, Karthikeyan K. Endodontic management of a fused maxillary lateral incisor with a supernumerary tooth: a case report. J Endod. 2006;32(12):1217-1219.
doi pubmed - Al-Hezaimi K, Naghshbandi J, Simon JH, Oglesby S, Rotstein I. Successful treatment of a radicular groove by intentional replantation and Emdogain therapy. Dent Traumatol. 2004;20(4):226-228.
doi pubmed - da Silva Neto UX, Hirai VH, Papalexiou V, Goncalves SB, Westphalen VP, Bramante CM, Martins WD. Combined endodontic therapy and surgery in the treatment of dens invaginatus Type 3: case report. J Can Dent Assoc. 2005;71(11):855-858.
pubmed - Maghsoudlou A, Jafarzadeh H, Forghani M. Endodontic treatment of a maxillary central incisor with two roots. J Contemp Dent Pract. 2013;14(2):345-347.
doi pubmed - Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin North Am. 2008;52(4):825-841, vii.
doi pubmed - Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011;44(11):990-999.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.