

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website https://www.jocmr.org |
Original Article
Volume 12, Number 11, November 2020, pages 724-733
Initial Acute Decline in Estimated Glomerular Filtration Rate After Sodium-Glucose Cotransporter-2 Inhibitor in Patients With Chronic Kidney Disease
Seigo Sugiyamaa, j, k, Akira Yoshidab, Kunio Hieshimac, Noboru Kurinamid, Katsunori Jinnouchie, f, Motoko Tanakag, Tomoko Suzukia, Fumio Miyamotoh, Keizo Kajiwaraa, d, Tomio Jinnouchia, d, Hideaki Jinnouchia, i, j
aCardiovascular Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
bPharmacology Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
cInfectious Disease Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
dObesity Treatment Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
eGastroenterology Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
fHemodialysis Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
gDepartment of Nephrology, Akebono Clinic, Kumamoto, Japan
hOphthalmology Division, Diabetes Care Center, Jinnouchi Hospital, Kumamoto, Japan
iDivision of Preventive Cardiology, Department of Cardiovascular Medicine, Kumamoto University Hospital, Kumamoto, Japan
jSeigo Sugiyama and Hideaki Jinnouchi contributed equally to this study.
kCorresponding Author: Seigo Sugiyama, Cardiovascular Division, Diabetes Care Center, Jinnouchi Hospital, 6-2-3 Kuhonji, Chuo-ku, Kumamoto City 862-0976, Japan
Manuscript submitted September 16, 2020, accepted September 22, 2020, published online November 3, 2020
Short title: Initial eGFR Drop by SGLT2 Inhibitor in CKD
doi: https://doi.org/10.14740/jocmr4351
| Abstract | ▴Top |
Background: Renal function deterioration accompanied by an acute decrease in estimated glomerular filtration rate (eGFR) was observed early after starting sodium-glucose cotransporter-2 inhibitor (SGLT2i) therapy. It is unclear how much and how frequently the initial acute decline in eGFR (IAD-eGFR) would occur after SGLT2i administration, and the effects of IAD-eGFR on subsequent renal function are unknown in type 2 diabetes mellitus (T2DM) patients with chronic kidney disease (CKD).
Methods: We retrospectively recruited T2DM patients with CKD (stage 3b; 30 ≤ eGFR < 45 mL/min/1.73 m2) and who were newly treated with add-on SGLT2i. We further investigated the effects of SGLT2i therapy on eGFR early after starting treatment (1 - 3 months) and after 6 months of treatment. We examined the factors associated with a large IAD-eGFR (≥ 10%) using logistic regression analyses.
Results: Eighty-seven patients (male, 74.7%; mean age, 69.8 years; median hemoglobin A1c, 7.3%; mean eGFR, 37.8 mL/min/1.73 m2) were analyzed. The mean minimum eGFR early after SGLT2i administration was 34.9 mL/min/1.73 m2, which was significantly lower than before treatment (mean, -7.7%). Seventy patients (80.5%) had IAD-eGFR, and 36 patients (41.4%) had a large IAD-eGFR (≥ 10%). Overall, the mean eGFR was 38.2 at 6 months after starting SGLT2i administration. In patients with a large IAD-eGFR (≥ 10%), the eGFR decreased by 72.2% at 6 months to 35.5 mL/min/1.73 m2, showing a significant decline from the pretreatment value. In patients without a large IAD-eGFR, eGFR increased by 66.7% at 6 months to 40.0 mL/min/1.73 m2. Multiple logistic regression analysis showed that patients with a large IAD-eGFR had a significant association with a high estimated daily salt intake.
Conclusions: SGLT2i treatment frequently induced a significant decrease in eGFR early after starting therapy, but eGFR tended to recover after 6 months in T2DM patients with CKD stage 3b. A large IAD-eGFR (≥ 10%) caused by SGLT2i may lead to subsequent deterioration in renal function, and it was significantly associated with a higher estimated daily salt intake. These results suggest that a more effective renoprotective therapeutic strategy using SGLT2i may be implemented by avoiding the occurrence of a large IAD-eGFR. Further prospective studies are warranted.
Keywords: Sodium-glucose cotransporter-2 inhibitors; Estimated glomerular filtration rate; Chronic kidney disease; Initial acute decline in eGFR; Type 2 diabetes mellitus; Renoprotection; Estimated daily salt intake; Tubuloglomerular feedback
| Introduction | ▴Top |
Diabetic nephropathy/diabetic kidney disease associated with type 2 diabetes mellitus (T2DM) is a serious medical problem that may be a causative factor for end-stage renal disease (ESRD) and induction to hemodialysis therapy [1]. In the treatment of T2DM patients with chronic kidney disease (CKD), adequate glycemic control and the intensive and integrated renal protection therapy using angiotensin converting enzyme-inhibitors, angiotensin-II receptor blockers, and other medications with renoprotective effects are required to avoid ESRD [2]. Recently, renoprotective effects of sodium-glucose cotransporter-2 inhibitors (SGLT2is) were reported in large clinical trials [3-5] and in real clinical practice [6]. However, in CKD-T2DM patients with reduced estimated glomerular filtration rate (eGFR), aggressive administration of SGLT2i is not recommended because of its attenuated hypoglycemic effects. Renoprotective effects by SGLT2i therapy are a desired result even in T2DM patients with reduced eGFR, but the clinical efficacy of SGLT2is has not been established. Recently, we have shown that additional administration of SGLT2i to T2DM patients with CKD stages 3b-4 could exert renoprotective effects of significantly attenuating annual eGFR decline and significantly reducing proteinuria excretion [7]. In the future, it could be postulated that SGLT2i therapy may be a beneficial consideration in T2DM patients with CKD with reduced eGFR from the viewpoint of renal protection.
Previous clinical studies have reported the presence of “initial acute decline in eGFR (IAD-eGFR),” which occurs in the early phase (1 - 3 months) after starting SGLT2i administration [8, 9]. In diabetes, abnormal tubuloglomerular feedback (TGF) by augmented reabsorption of glucose/sodium in the proximal tubule causes dilation of the afferent glomerular arteriole, resulting in increased intra-glomerular pressure and glomerular hyperfiltration. SGLT2i treatment produces IAD-eGFR by reducing glomerular hyperfiltration via improving TGF [10]. Although SGLT2i therapy produces IAD-eGFR, it is thought that the subsequent rate of eGFR decrease (slope) becomes slower and exerts renoprotective effects in the long term [11]. In many CKD-T2DM patients, rapid eGFR decline is often observed, and the already reduced eGFR could further be lowered by IAD-eGFR after starting SGLT2i therapy, which may induce sudden and additional renal functional deterioration. Thus, physicians could hesitate to start SGLT2i administration.
Currently, it is unknown how much and how frequently IAD-eGFR occurs in T2DM patients with CKD stage 3b in real clinical practice. In addition, the effects of IAD-eGFR on subsequent renal function are also unknown. Here, we retrospectively investigated the IAD-eGFR induced by starting SGLT2i therapy in T2DM patients with CKD stage 3b in a routine real clinical setting.
| Materials and Methods | ▴Top |
Study population and study protocol
Based on clinical information from hospital medical records, we retrospectively identified Japanese outpatients with T2DM who were newly treated with SGLT2i between April 2014 and December 2019 in the Diabetes Care Center at Jinnouchi Hospital, Kumamoto, Japan. Among them, we selected patients who also had moderate renal impairment defined as CKD stage 3b (30 ≤ eGFR < 45 mL/min/1.73 m2) at the initiation of SGLT2i therapy. Finally, we selected patients with T2DM and moderate renal impairment who continued to use SGLT2i for at least 6 months and whose acute phase eGFR data during the initial 3 months after SGLT2i therapy were available to analyze. The exclusion criteria were as follows: type 1 DM, unstable cardiovascular diseases, active inflammation, autoimmune diseases, infectious diseases, severe liver disease, dementia, and cancer. Patients with newly diagnosed DM who were not undergoing any form of treatment and those with ketosis were also excluded. This cohort consisted of patient data obtained from a routine clinical database at Jinnouchi Hospital. We primarily investigated the initial acute changes in eGFR after SGLT2i therapy. If there were two or three eGFR data during the initial 3 months after SGLT2i therapy, we selected the lowest eGFR value as the representative initial acute-phase eGFR data. The primary outcome was a quantitative assessment of the initial acute changes in eGFR (mL/min/1.73 m2) and percent changes in eGFR. We also analyzed eGFR at 6 months after SGLT2i therapy. This was a retrospective, observational, single-arm, and single center study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Human Ethics Review Committee of Jinnouchi Hospital (2019-11-(1)) Signed informed consent was obtained from each patient. The study was registered under the University Hospital Medical Information Network (UMIN) protocol registration system (ID: UMIN R000045509).
Assessments and measurement of clinical parameters
We collected clinical information pertaining to medical treatments, complications, family history, and medical history. We also collected data on body weight, height, blood pressure, and pulse rate. Analyses of blood and urine were conducted in the hospital laboratory to measure hemoglobin (Hb), hematocrit, blood glucose, HbA1c, albumin, creatinine, blood urea nitrogen, urinary protein, sodium, and urinary creatinine. For the semi-quantitative assessments of urinary protein excretion (urinary protein concentration > 30 mg/dL) and hematuria (> 10 red blood cells/µL), we also examined the results of a dipstick urine test. The eGFR (mL/min/1.73 m2) was calculated using the formula from the Japanese Society of Nephrology [12] before SGLT2i therapy (1 year before) at the initiation of SGLT2i therapy and after therapy (1 - 6 months). We calculated the pre-treatment annual changes, the initial acute changes, and the post-treatment 6 months changes in eGFR by the following formula: pretreatment annual eGFR change = (eGFR at starting SGLT2i therapy) - (eGFR at 1-year ago from starting SGLT2i therapy); initial acute eGFR change = (minimum eGFR during initial 3 months after SGLT2i therapy) - (eGFR at starting SGLT2i therapy); post-treatment 6 months eGFR change = (eGFR after 6 months SGLT2i therapy) - (eGFR at starting SGLT2i therapy).
Daily salt intake was calculated using the Tanaka method [13]; it was estimated based on the calculation of 24-h sodium and creatinine levels from spot urine samples. The Tanaka method is recommended in the Japanese hypertension guideline 2019 because of its convenience and reliability. Estimated daily salt intake (g/day) was calculated using the following formula: 24-h urinary salt excretion (g/day) = 0.0585 × 21.98× (UNa (mEq/L)/UCr (mg/L) × (-2.04 × age + 14.89 × weight (kg) + 16.14 × height (cm) - 2244.45))0.392. In this formula, sodium and creatinine concentrations were determined from the spot urine samples that were collected in the morning.
Measurement of body component
Elementary body composition, including total fat mass, total body muscle mass, total body water (ToBW), extracellular water (ECW), intracellular water (ICW), and skeletal muscle mass (SMM), was measured using a direct segmental multi-frequency bioelectrical impedance analyzer (InBody770) [14]. This analyzer processes 30 impedance measurements by using six different frequencies (1, 5, 50, 250, 500, and 1000 kHz) at each of five segments of the body (right arm, left arm, trunk, right leg, and left leg) and 15 reactance measurements using tetrapolar eight-point tactile electrodes at three different frequencies (5, 50, and 250 kHz) at each of the five body segments (right arm, left arm, trunk, right leg, and left leg) [15, 16].
Statistical analyses
The primary endpoint of the present study was treatment-induced IAD-eGFR. We analyzed the significant acute reduction in eGFR during the initial phase after SGLT2i therapy. To investigate the effects of SGLT2i therapy on eGFR, we compared values of eGFR at the initiation of SGLT2i therapy (baseline) during the initial 3 months and at 6 months after starting therapy. We also analyzed the percent changes in the initial acute change in eGFR compared with the eGFR values when SGLT2i therapy was started (baseline). Percent changes in eGFR were calculated by the following formula: percent change in initial acute change in eGFR (%) = initial acute eGFR change × 100/eGFR at starting SGLT2i therapy (baseline) Because the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) study demonstrated an approximate 10% decline in eGFR during the initial phase of SGLT2i therapy [4], patients with a large IAD-eGFR were tentatively defined as having a larger IAD-eGFR ≥ 10.0% in our present study. We compared clinical backgrounds, complications, medications, body weight, body mass index (BMI), blood pressure, pulse rate, body components, and estimated daily salt intake between patients with or without the large IAD-eGFR. We also investigated the effects of the presence of a large IAD-eGFR (≥ 10%) on the 6-month eGFR change. Data pertaining to normally distributed continuous variables (determined by the Shapiro-Wilk test) are presented as the mean (standard deviation (SD)), while those of continuous variables with a skewed distribution are presented as median values (interquartile range). Differences in the baseline characteristics of the two groups were analyzed using the Student’s t-test, the Mann-Whitney U test, or Fisher’s exact test for categorical data, as appropriate. The serial changes in eGFR and differences of the paired data in each group were analyzed by Student’s paired t-test. To determine the factors that were associated with a large IAD-eGFR (≥ 10%), a logistic regression analysis was used to evaluate the association between a large IAD-eGFR (≥ 10%) and baseline clinical variables, including the age, sex, BMI, HbA1c, casual plasma glucose, diabetes duration, medications, complications, Hb, albumin, blood pressure, pulse rate, and several measurements of body composition. Associations between groups and all other parameters were analyzed first by a univariate logistic regression analysis. This was followed by a multivariate logistic regression analysis using the forced inclusion model with all significant factors in the univariate logistic regression analysis (P < 0.05), and the Hosmer-Lemeshow goodness-of-fit statistic was calculated. A P value < 0.05 was considered to be statistically significant. Statistical analyses were performed using the Statistical Package for Social Sciences software program, version 23 (SPSS Inc., IBM, Tokyo, Japan).
| Results | ▴Top |
Patient baseline clinical parameters
A total of 1,553 Japanese stable T2DM patients who were newly treated with SGLT2i were initially identified, 123 (7.9%) of whom had moderate CKD (stage 3b) at the initiation of SGLT2i therapy. Thirty-six patients were excluded because the eGFR acute phase data during the initial 3 months after starting SGLT2i therapy were not available or they were not treated with SGLT2is for over 6 months as of December 2019. We retrospectively analyzed a final cohort of 87 patients, whose baseline clinical parameters are shown in Table 1. The mean age was 69.8 years, 74.7% were male, mean duration of T2DM was 21.7 years, and mean BMI was 26.9 kg/m2. Overall, more than 90% of patients had complications of hypertension and dyslipidemia, 40.2% of had a history of cerebrovascular/cardiovascular diseases, and 60.9% of patients had diabetic retinopathy. The median HbA1c value was 7.3%, and 32.2% of patients were treated with metformin, while 60.9% were treated with insulin. The attending physicians at Jinnouchi Hospital started SGLT2i at their own discretion to improve glycemic control, and the starting treatment doses of SGLT2i were regularly established in Japanese clinical practice (dapagliflozin, 5 mg/day; empagliflozin, 10 mg/day; canagliflozin, 100 mg/day; ipragliflozin, 50 mg/day; luseogliflozin, 2.5 mg/day; and tofogliflozin, 20 mg/day). Mean eGFR was 37.8 mL/min/1.73 m2 at the initiation of SGLT2i therapy. Additionally, 44.8% of patients had proteinuria (urinary protein concentration > 30 mg/dL), and 32.3% had hematuria (> 10 red blood cells/µL). Urinary albumin was not measured in the present study.
 Click to view | Table 1. Clinical Characteristics of Patients |
Initial acute changes in eGFR after starting SGLT2i therapy
Overall, eGFR significantly decreased from 37.8 ± 4.5 to 34.9 ± 5.8 mL/min/1.73 m2 during the initial acute phase after staring SGLT2i therapy (Fig. 1). The mean value of the initial acute change in eGFR was -2.9 mL/min/1.73 m2, and the maximum value of initial acute change in eGFR was -13.1 mL/min/1.73 m2. No patient acutely developed ESRD (eGFR less than 15 mL/min/1.73 m2) after the start of SGLT2i therapy in the present study. Figure 2 shows the distribution of the percent changes in the initial acute change in eGFR after SGLT2i therapy. The mean percent change in the initial acute change in eGFR was -7.7%, and the maximum percent change in the initial acute change in eGFR was -33.2%. During the initial acute phase after SGLT2i therapy, eGFR decreased in 80.5% of total patients, and we first found that 19.5% of patients with CKD stage 3b did not have any reduction in eGFR (Figs. 3a, 4). We found that 39.1% of patients (n = 34) had mild IAD-eGFR (0-10%), 41.4% of patients (n = 36) had a large IAD-eGFR ≥ 10% (Fig. 3b), and 10.3% of patients (n = 9) had a severe IAD-eGFR ≥ 20% in the present study (Fig. 4).
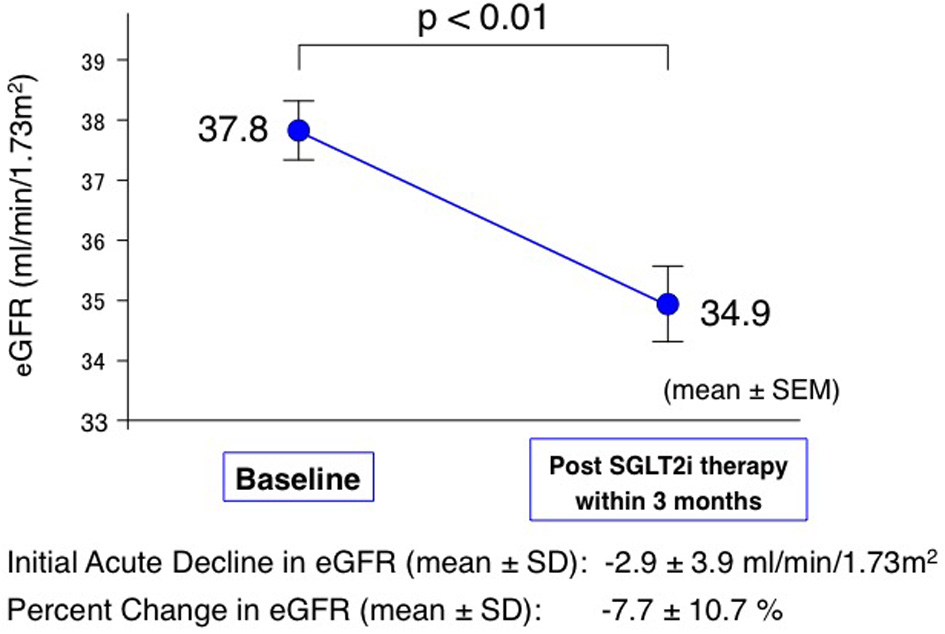 Click for large image | Figure 1. IAD-eGFR after starting SGLT2i therapy in T2DM patients with CKD stage 3b. The line graph indicates serial changes in eGFR before and early after treatment with SGLT2is. The serial changes in eGFR were analyzed by Student’s paired t-test (n = 87, P < 0.01). SGLT2i: sodium-glucose cotransporter-2 inhibitor; eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SEM: standard error of mean; SD: standard deviation. |
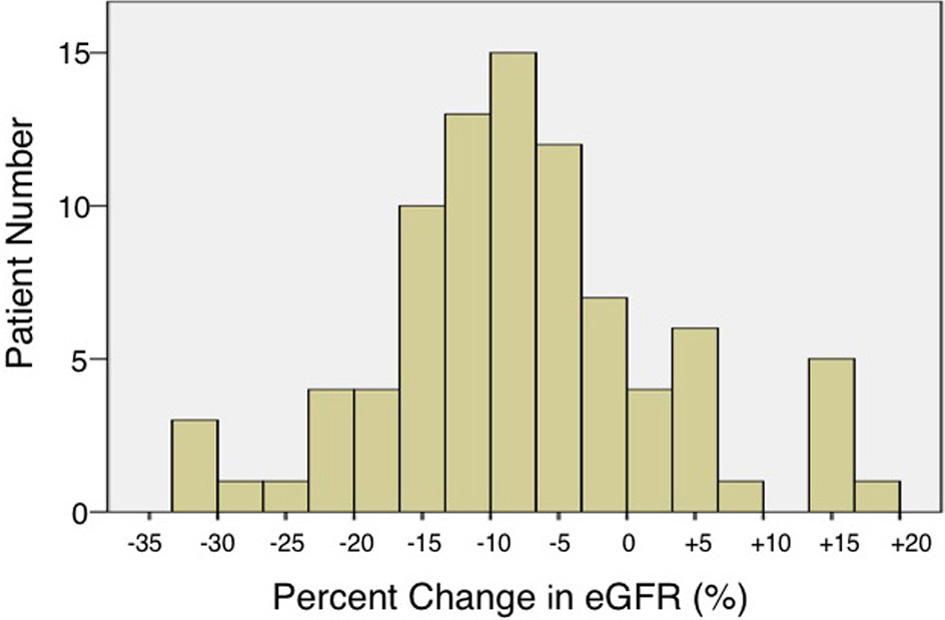 Click for large image | Figure 2. Distribution of percent changes in IAD-eGFR after starting SGLT2i therapy in T2DM patients with CKD stage 3b. Bar histogram indicates patient number in each percent change in eGFR. eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SGLT2i: sodium-glucose cotransporter-2 inhibitor; T2DM: type 2 diabetes mellitus; CKD: chronic kidney disease. |
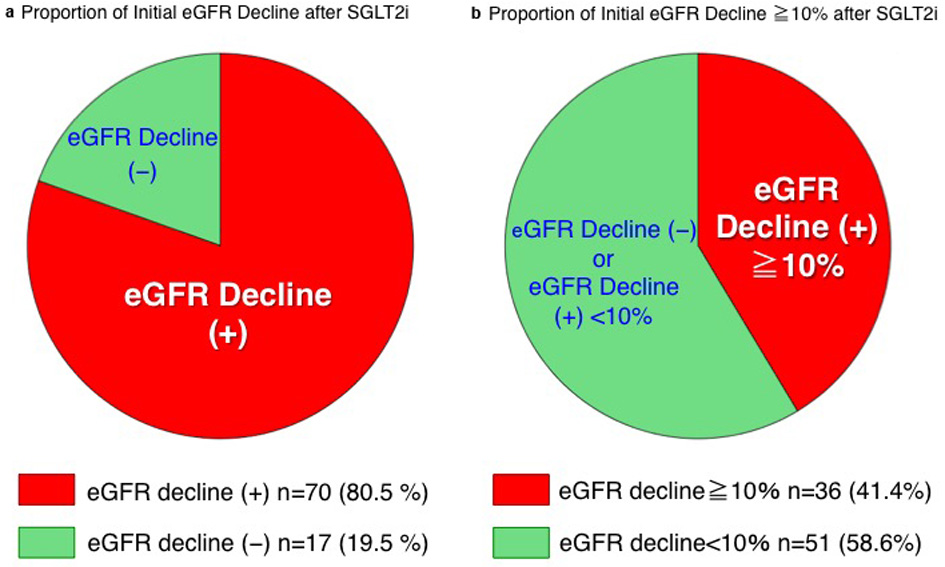 Click for large image | Figure 3. Proportion of IAD-eGFR after starting SGLT2i therapy in T2DM patients with CKD stage 3b. (a) Proportion of any eGFR decline in and (b) proportion of large eGFR decline more than 10%. eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SGLT2i: sodium-glucose cotransporter-2 inhibitor; T2DM: type 2 diabetes mellitus; CKD: chronic kidney disease. |
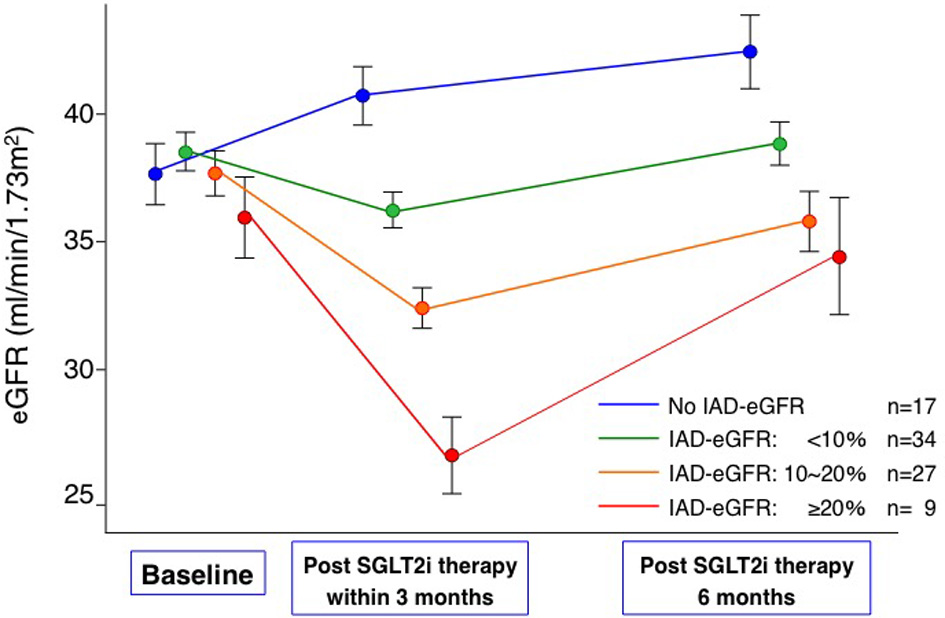 Click for large image | Figure 4. Time course effects of IAD-eGFR after starting SGLT2i therapy on levels of 6 months eGFR in T2DM patients with CKD stage 3b. The line graph indicates serial changes in eGFR before and after treatment with SGLT2is according to the degree of IAD-eGFR. eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SGLT2i: sodium-glucose cotransporter-2 inhibitor; T2DM: type 2 diabetes mellitus; CKD: chronic kidney disease. |
Effects of IAD-eGFR on eGFR 6 months after starting SGLT2i therapy
Overall, for T2DM patients with CKD, eGFR did not significantly decrease from the start of SGLT2i to 6 months (mean eGFR, 37.8 to 38.2 mL/min/1.73 m2, P = 0.49). In patients with any IAD-eGFR (n = 70), the mean eGFR value significantly decreased from 37.9 ± 4.5 mL/min/1.73 m2 at baseline to 33.5 ± 5.3 mL/min/1.73 m2 in the acute phase (P < 0.01), and eGFR almost recovered to 37.1 ± 5.9 mL/min/1.73 m2 at 6 months. In patients with a mild IAD-eGFR (0-10%) (n = 34), the mean eGFR value significantly decreased in the acute phase (P < 0.01), and eGFR completely recovered to the baseline levels at 6 months. In patients with a large IAD-eGFR (10-20%) (n = 27) and severe IAD-eGFR (≥ 20%) (n = 9), eGFR significantly decreased in the acute phase (p < 0.01), and eGFR did not fully recover to the baseline levels at 6 months (Fig. 4). In contrast, the mean eGFR value significantly increased from 37.7 ± 4.9 mL/min/1.73 m2 at baseline to 40.7 ± 4.7 mL/min/1.73 m2 in the acute phase (P < 0.01), and eGFR further increased to 42.4 ± 5.9 mL/min/1.73 m2 at 6 months in patients without any IAD-eGFR (n = 17, Fig. 4). Figure 5 demonstrates the mean change in eGFR over time in the two groups with or without a large IAD-eGFR (≥ 10%). In patients with a large IAD-eGFR (≥ 10%), mean values of eGFR significantly decreased from 37.2 to 31.0 mL/min/1.73 m2 (P < 0.01) in the initial acute phase, while patients without a large IAD-eGFR (no IAD-eGFR or mild IAD-eGFR) did not have significant reduction in eGFR and could successfully maintain eGFR levels (mean; 38.2 to 37.7 mL/min/1.73 m2) in the initial acute phase after SGLT2i therapy (Fig. 5). When we retrospectively investigated the effects of a large IAD-eGFR (≥ 10%) on eGFR at 6 months after SGLT2i therapy, eGFR significantly decreased from baseline values in patients with a large IAD-eGFR (≥ 10%) but not in those without a large IAD-eGFR (Fig. 5). eGFR values were significantly elevated from baseline levels in patients without a large IAD-eGFR (Fig. 5). At 6 months after SGLT2i therapy, we found a significant difference in eGFR between these two groups (Fig. 5). Overall, 43 patients (49.4%) demonstrated a reduction in eGFR at 6 months after baseline (Fig. 6). The frequency of patients with any reduction in the 6-month eGFR from baseline levels was significantly greater in patients with a large IAD-eGFR (≥ 10%) in 72.2% compared with that of those without a large IAD-eGFR in 33.3% (P < 0.01) (Fig. 6).
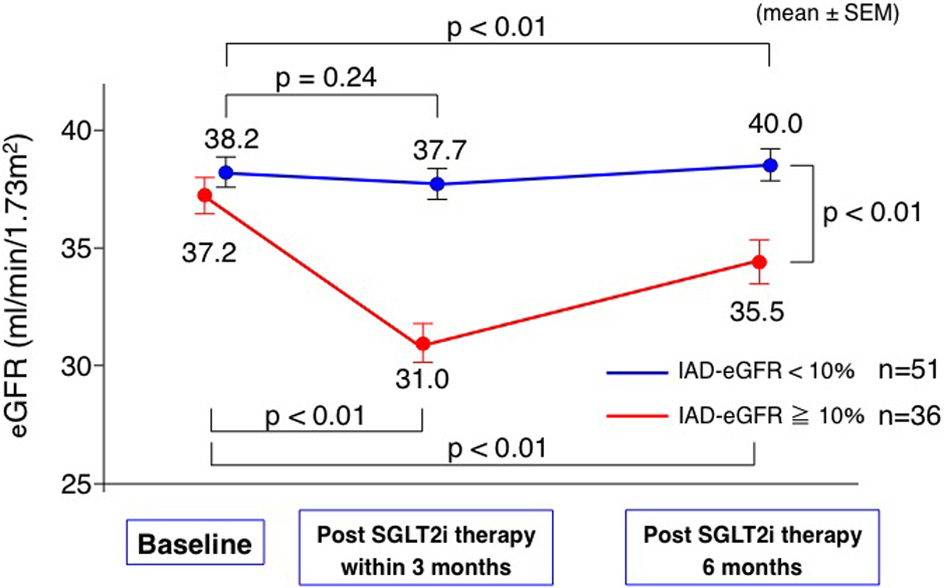 Click for large image | Figure 5. Time course effects of large IAD-eGFR (≥ 10%) after starting SGLT2i therapy on levels of 6 months eGFR in T2DM patients with CKD stage 3b. The line graph indicated serial changes in eGFR before and after treatment with SGLT2is according to the presence or absence of large IAD-eGFR (≥ 10%). eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SGLT2i: sodium-glucose cotransporter-2 inhibitor; T2DM: type 2 diabetes mellitus; CKD: chronic kidney disease; SEM: standard error of mean. |
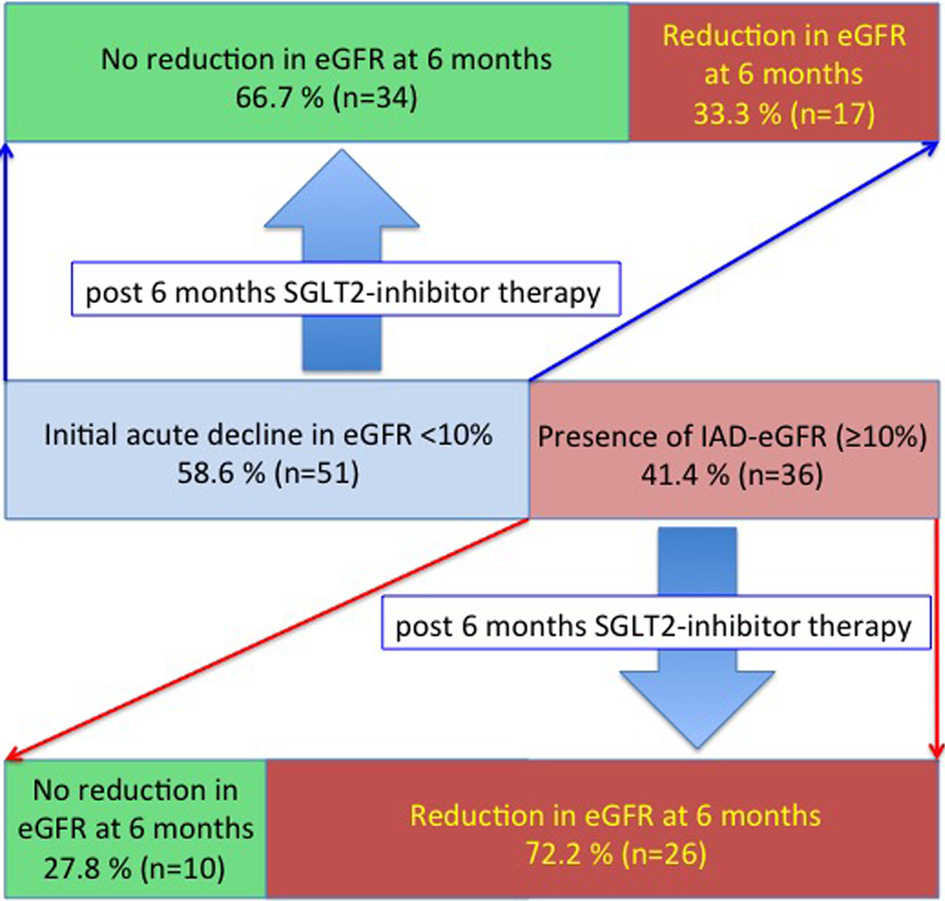 Click for large image | Figure 6. Effects of large IAD-eGFR (≥ 10%) after starting SGLT2i therapy on the changes in 6 months eGFR in T2DM patients with CKD stage 3b. eGFR: estimated glomerular filtration rate; IAD-eGFR: initial acute decline in eGFR; SGLT2i: sodium-glucose cotransporter-2 inhibitor; T2DM: type 2 diabetes mellitus; CKD: chronic kidney disease. |
Comparison of baseline parameters in patients with or without a large IAD-eGFR (≥ 10%)
When we divided the patients into two groups to compare the patients with or without a large IAD-eGFR (≥ 10%), there were no significant differences in age, gender, body weight, BMI, complications, medications, blood pressure, pulse rate, ToBW, or total body fat mass between the groups (Tables 1, 2). Baseline values of eGFR, HbA1c, and casual plasma glucose tended to be lower, and the diabetes duration tended to be longer in the group with a large IAD-eGFR (≥ 10%) (Table 1). The percentage of proteinuria was significantly higher in patients with a large IAD-eGFR (≥ 10%) (Table 1). The Hb and serum albumin concentration were significantly lower, and the amounts of estimated daily salt intake and the percent of ECW to ToBW were significantly higher in patients with a large IAD-eGFR (≥ 10%) (Table 2).
Click to view | Table 2. Clinical and Body Composition Parameters Before Treatment With SGLT2i |
Logistic regression analysis for a large IAD-eGFR (≥ 10%)
A univariate logistic regression analysis with various baseline parameters showed that the presence of proteinuria, estimated daily salt intake, percentage of ECW to ToBW, serum albumin, and Hb were significantly correlated with occurrence of a large IAD-eGFR (≥ 10%) (Table 3). Forced inclusion of multivariate logistic regression analysis with all the above significant factors showed that only an estimated daily salt intake was significantly correlated with a large IAD-eGFR (≥ 10%) (odds ratio: 1.334; 95% confidence interval: 1.023 to 1.738; P = 0.033). The Hosmer-Lemeshow statistic was appropriate (P = 0.87).
Click to view | Table 3. Logistic Regression Analysis for a Large IAD-eGFR More Than 10% of Among Pretreatment Factors |
| Discussion | ▴Top |
SGLT2i treatment in T2DM patients with CKD stage 3b caused a decrease in eGFR in many patients (over 80%) in the early phase after the start of treatment at a Japanese outpatient clinic, and this decrease in eGFR was a significant change. A large IAD-eGFR (≥ 10%) due to SGLT2i was present in 41.1% of patients, and the occurrence of a large IAD-eGFR (≥ 10%) was significantly associated with a highly estimated daily salt intake before treatment. Furthermore, eGFR at 6 months after SGLT2i treatment was significantly lower than that before treatment in patients with a large IAD-eGFR (≥ 10%).
It is presumed that hyperglycemia and increased glucose urine induce SGLT2 up-regulation in the proximal tubule and abnormal tubuloglomerular feedback (TGF), and this TGF abnormality causes glomerular overload due to glomerular hypertension and hyper-filtration, leading to renal damage [10]. Glomerular hyper-filtration in diabetes is considered to be the causative condition of renal damage in the early stage of diabetes and in patients whose eGFR levels were relatively maintained [17]. However, it is unclear how much glomerular hyper-filtration is present in patients with impaired renal function with already reduced eGFR and how it is involved in subsequent changes in renal function. Although it has been reported that SGLT2i treatment causes IAD-eGFR in large-scale clinical trials to date [4, 5, 8, 9], most of the subjects examined in these studies were patients with normal eGFR or preserved eGFR. IAD-eGFR in affected patients with reduced eGFR is still unknown. A recent small-scale prospective study reported that IAD-eGFR in CKD stage 3b patients was not particularly observed and did not cause a significant decrease [18], and a sub-analysis of the CREDENCE study showed that IAD-eGFR was not significantly observed, and they reported that the changes in eGFR were the smallest in CKD stage 3b patients [19]. In the real world data from our daily clinical practice, IAD-eGFR was observed in more than 80% of CKD-3b diabetic patients, and a significant decrease in eGFR (-7.7%) was confirmed in the entire population. This suggests that early eGFR changes after SGLT2i treatment in patients with impaired renal function who participated in a prospective clinical study may differ from eGFR responses in the real world clinical patients. Because IAD-eGFR was found in many patients with renal dysfunction (CKD stage 3b) in the present study, there is a hyper-filtration state in each residual glomerulus even in patients with advanced renal dysfunction. These results also suggest that SGLT2i treatment may lead to a reduction in glomerular hyper-filtration even in patients with advanced CKD. IAD-eGFR is considered to be a reversible and beneficial phenomenon because SGLT2i and correction of the TGF abnormality cause a reduction in glomerular overload in diabetes [17]. However, based on the results of this study in actual clinical practice, in some patients with CKD stage 3b with already decreased eGFR, a significantly large decrease in eGFR occurs during the early phase of SGLT2i treatment, which leads to a further decrease in eGFR with long-term therapy. We considered that it should be necessary to carefully observe and treat CKD patients after starting SGLT2i.
Our present study showed for the first time that approximately 20% of CKD stage 3b diabetic patients did not have IAD-eGFR due to SGLT2i treatment (No-IAD-eGFR). In this patient group, eGFR after SGLT2i treatment was unexpectedly increased from the early phase after the start of treatment. In patients with No-IAD-eGFR, it is speculated that glomerular hyper-filtration did not already exist. However, SGLT2i treatment resulted in renal protection by reducing tubulointerstitial damage [6] and metabolic stress in proximal tubules [20], resulting in eGFR elevation. We believe that this increase in eGFR does not mean that the SGLT2i treatment causes further glomerular hyper-filtration, but rather, it is considered to be a recovery and improvement in renal function by SGLT2i treatment, which might be a beneficial phenomenon for renal protection. Because there are No-IAD-eGFR patients, this indicates that IAD-eGFR is not an essential phenomenon that is induced by SGLT2i treatment. This suggests that there is a clinical possibility that the development of IAD-eGFR can be avoided by some clinical strategies when starting SGLT2i.
Before conducting this retrospective study, we expected that initiation of SGLT2i treatment in patients with poor glycemic control and hyperglycemia would result in a large IAD-eGFR, but HbA1c and blood glucose levels were not significantly associated with a large IAD-eGFR. Here, we have revealed that large IAD-eGFR is significantly associated with excessive salt intake before SGLT2i treatment in the results of a multivariate logistic regression analysis. It has been proposed that excessive salt intake is involved in deterioration of renal function [21]. Because SGLT2i suppresses glucose and sodium reabsorption in the proximal tubules to the same extent, it has been suggested that glomerular hyper-filtration that is caused by excessive salt intake could be also be improved by SGLT2i treatment [17]. If sufficient salt-reducing instructions and low-salt diet therapy are achieved before starting SGLT2i treatment, it may be possible to avoid development of large IAD-eGFR, which may lead to more effective renal protection treatment. Expected results should be verified by future prospective research.
In CKD - stage 3b patients, residual renal function has already decreased to 50% or less compared with that of healthy subjects and avoiding ESRD requires intensive treatment to minimize the decrease in the eGFR slope in the future. Diabetics with an annual eGFR decline of 7.5% or more have a poor renal prognosis [22]. In the present study, we found that SGLT2i-induced IAD-eGFR showed a 7.7% decrease in eGFR within 3 months after starting drug administration. After starting SGLT2i treatment, an acute and transient eGFR decline has been observed in the early stage, but thereafter, the decline in the eGFR slope gradually decreased and became flat; this shows that there is a renal protective effect with long-term treatment [11]. From our present study, IAD-eGFR was also observed in many patients with CKD stage 3b, but thereafter, the eGFR level increased and tended to recover for 6 months after the start of treatment. When IAD-eGFR was less than 10%, the eGFR level decreased transiently in the early stage of treatment, but after 6 months, it was almost completely restored to the level at the start of treatment. However, in patients with a large IAD-eGFR (≥ 10%), a recovery trend was observed starting from the early decrease in the eGFR value towards 6 months, but sufficient recovery to the value at the start of treatment was not obtained, and the eGFR levels at 6 months were significantly lower than those at the start of treatment. In the future, it may be useful to consider potential therapeutic plans to start SGLT2i treatment to keep IAD-eGFR within 10%.
Limitations
This study had several limitations including the small sample size, a relatively short study period, a retrospective study design, and possible bias in patient selection at the single center. There is selection bias in this study because the proportion of patients with SGLT2i relative to all diabetic patients was extremely low. The present study was retrospectively designed, and the study protocol was not prospectively controlled. Thus, the evidence level of this study is not high. Further prospective, more detailed, larger, and longer studies focusing on patients with CKD stage 3b with a multicenter design are required to validate the effects of SGLT2i therapy on IAD-eGFR and renal function as shown herein. The detailed molecular mechanisms underlying the SGLT2i-induced improvements in renal function could not be determined in the present clinical study and should be investigated in future studies. Further prospective studies are needed to investigate the effect of the pretreatment intervention to salt intake on the occurrence of IAD-eGFR and further renal function.
Conclusions
SGLT2i treatment in T2DM patients with CKD stage 3b caused a significant decrease in eGFR in many patients during the early phase after the initiation of the treatment. Most of the IAD-eGFRs were transient and showed a tendency to recover after 6 months, but in patients with a large IAD-eGFR (≥ 10%), eGFR significantly decreased at 6 months after therapy, and a significant association with a highly estimated daily salt intake before SGLT2i treatment was observed. It is suggested that avoiding a large IAD-eGFR in the early phase of SGLT2i treatment may lead to successful renal protection that could maintain eGFR levels. This could lead to more effective renoprotective therapy with SGLT2i in the future.
Financial Disclosure
None to declare.
Conflict of Interest
Dr. Seigo Sugiyama is on the Speaker’s Bureau of MSD, Inc., and AstraZeneca Pharmaceuticals LP, Ono Pharmaceutical Co., Ltd., and Bayer Yakuhin Ltd. Dr. Hideaki Jinnouchi has received consultant fees from Sanofi U.S., Novo Nordisk, Inc., and Eli Lilly Japan K.K. Dr. Hideaki Jinnouchi is also on the Speaker’s Bureau of MSD, Inc., Astellas Pharma US, Inc., Sanofi U.S., Novo Nordisk Pharma, Ltd., Taisho Pharmaceutical, Co., Ltd. Daiichi-Sankyo Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Eli Lilly Japan K.K., Boehringer Ingelheim Pharmaceuticals, Inc., Takeda Pharmaceutical Company Limited, and AstraZeneca Pharmaceuticals LP. All other authors declare that they have no conflict of interest.
Informed Consent
Signed informed consent was obtained from each patient.
Author Contributions
All the authors contributed to study conception and design. SS, AY, KH, NK, KJ, TS, FM, KK, and HJ acquired the data. SS, AY, MT, and HJ analyzed and interpreted data. SS and HJ drafted the manuscript. All the authors involved in critical revisions.
Data Availability
The authors declare that the data supporting the findings of this study are available within the article.
| References | ▴Top |
- Duru OK, Middleton T, Tewari MK, Norris K. The landscape of diabetic kidney disease in the United States. Curr Diab Rep. 2018;18(3):14.
doi pubmed - Muskiet MHA, Wheeler DC, Heerspink HJL. New pharmacological strategies for protecting kidney function in type 2 diabetes. Lancet Diabetes Endocrinol. 2019;7(5):397-412.
doi - Cherney DZI, Zinman B, Inzucchi SE, Koitka-Weber A, Mattheus M, von Eynatten M, Wanner C. Effects of empagliflozin on the urinary albumin-to-creatinine ratio in patients with type 2 diabetes and established cardiovascular disease: an exploratory analysis from the EMPA-REG OUTCOME randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2017;5(8):610-621.
doi - Perkovic V, de Zeeuw D, Mahaffey KW, Fulcher G, Erondu N, Shaw W, Barrett TD, et al. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS Program randomised clinical trials. Lancet Diabetes Endocrinol. 2018;6(9):691-704.
doi - Mosenzon O, Wiviott SD, Cahn A, Rozenberg A, Yanuv I, Goodrich EL, Murphy SA, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE-TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606-617.
doi - Sugiyama S, Jinnouchi H, Kurinami N, Hieshima K, Yoshida A, Jinnouchi K, Tanaka M, et al. Impact of dapagliflozin therapy on renal protection and kidney morphology in patients with uncontrolled type 2 diabetes mellitus. J Clin Med Res. 2018;10(6):466-477.
doi pubmed - Sugiyama S, Jinnouchi H, Yoshida A, Hieshima K, Kurinami N, Jinnouchi K, Tanaka M, et al. Renoprotective effects of additional sglt2 inhibitor therapy in patients with type 2 diabetes mellitus and chronic kidney disease stages 3b-4: a real world report from a Japanese Specialized Diabetes Care Center. J Clin Med Res. 2019;11(4):267-274.
doi pubmed - Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, Johansen OE, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-334.
doi pubmed - Heerspink HJL, Karasik A, Thuresson M, Melzer-Cohen C, Chodick G, Khunti K, Wilding JPH, et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): a multinational observational cohort study. Lancet Diabetes Endocrinol. 2020;8(1):27-35.
doi - Vallon V, Thomson SC. The tubular hypothesis of nephron filtration and diabetic kidney disease. Nat Rev Nephrol. 2020;16(6):317-336.
doi pubmed - Wanner C, Heerspink HJL, Zinman B, Inzucchi SE, Koitka-Weber A, Mattheus M, Hantel S, et al. Empagliflozin and Kidney Function Decline in Patients with Type 2 Diabetes: A Slope Analysis from the EMPA-REG OUTCOME Trial. J Am Soc Nephrol. 2018;29(11):2755-2769.
doi pubmed - Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53(6):982-992.
doi pubmed - Tanaka T, Okamura T, Miura K, Kadowaki T, Ueshima H, Nakagawa H, Hashimoto T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J Hum Hypertens. 2002;16(2):97-103.
doi pubmed - Malavolti M, Mussi C, Poli M, Fantuzzi AL, Salvioli G, Battistini N, Bedogni G. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21-82 years. Ann Hum Biol. 2003;30(4):380-391.
doi pubmed - Kurinami N, Sugiyama S, Yoshida A, Hieshima K, Miyamoto F, Kajiwara K, Jinnouchi T, et al. Correlation of body muscle/fat ratio with insulin sensitivity using hyperinsulinemic-euglycemic clamp in treatment-naive type 2 diabetes mellitus. Diabetes Res Clin Pract. 2016;120:65-72.
doi pubmed - Sugiyama S, Jinnouchi H, Kurinami N, Hieshima K, Yoshida A, Jinnouchi K, Nishimura H, et al. Dapagliflozin reduces fat mass without affecting muscle mass in type 2 diabetes. J Atheroscler Thromb. 2018;25(6):467-476.
doi pubmed - Tonneijck L, Muskiet MH, Smits MM, van Bommel EJ, Heerspink HJ, van Raalte DH, Joles JA. Glomerular hyperfiltration in diabetes: mechanisms, clinical significance, and treatment. J Am Soc Nephrol. 2017;28(4):1023-1039.
doi pubmed - Matsuba I, Kawata T, Iemitsu K, Asakura T, Amemiya H, Ishikawa M, Ito S, et al. Effects of ipragliflozin on the development and progression of kidney disease in patients with type 2 diabetes: An analysis from a multicenter prospective intervention study. J Diabetes Investig. 2020.
doi pubmed - Jardine MJ, Zhou Z, Mahaffey KW, Oshima M, Agarwal R, Bakris G, Bajaj HS, et al. Renal, cardiovascular, and safety outcomes of canagliflozin by baseline kidney function: a secondary analysis of the CREDENCE randomized trial. J Am Soc Nephrol. 2020;31(5):1128-1139.
doi pubmed - Sano M, Goto S. Possible mechanism of hematocrit elevation by sodium glucose cotransporter 2 inhibitors and associated beneficial renal and cardiovascular effects. Circulation. 2019;139(17):1985-1987.
doi pubmed - Weir MR, Fink JC. Salt intake and progression of chronic kidney disease: an overlooked modifiable exposure? A commentary. Am J Kidney Dis. 2005;45(1):176-188.
doi pubmed - Nojima J, Meguro S, Ohkawa N, Furukoshi M, Kawai T, Itoh H. One-year eGFR decline rate is a good predictor of prognosis of renal failure in patients with type 2 diabetes. Proc Jpn Acad Ser B Phys Biol Sci. 2017;93(9):746-754.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.