

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Original Article
Volume 11, Number 6, June 2019, pages 447-451
Background Factors Determining the Introduction and Dosage of Insulin in Women With Gestational Diabetes Mellitus
Yuko Matsumotoa, Hodaka Yamadaa, c, Masashi Yoshidaa, Daisuke Suzukia, Rika Saikawaa, Misato Amamotoa, Shunsuke Funazakia, Isao Horiuchib, Kenjiro Takagib, Kazuo Haraa
aDepartment of Medicine, Division of Endocrinology and Metabolism, Jichi Medical University Saitama Medical Center, 1-847 Amanuma-cho, Omiya-ku, Saitama 330-8503, Japan
bPerinatal and Maternal Center of Saitama Medical Center, Jichi Medical University Saitama Medical Center, 1-847 Amanuma-cho, Omiya-ku, Saitama 330-8503, Japan
cCorresponding Author: Hodaka Yamada, Department of Medicine, Division of Endocrinology and Metabolism, Jichi Medical University Saitama Medical Center, 1-847 Amanuma-cho, Omiya-ku, Saitama 330-8503, Japan
Manuscript submitted March 22, 2019, accepted April 16, 2019
Short title: GDM and Factors for Insulin Therapy
doi: https://doi.org/10.14740/jocmr3824
| Abstract | ▴Top |
Background: Gestational diabetes mellitus (GDM) is a risk for perinatal complication, and appropriate diagnosis of and intervention in this condition are important. This study aimed to identify patient factors associated with introduction and dosage of insulin, which is the main drug for treatment of GDM.
Methods: In total, 114 patients who had been diagnosed with GDM at our hospital were included in this study. We retrospectively collected clinical parameters of GDM patients, including how many times positive glucose tolerance test results were obtained, whether insulin was introduced, dosage of insulin, body weight, and infant weight. Background factors differing between the insulin introduction and non-introduction groups of GDM patients and parameters associated with the insulin dosage were analyzed.
Results: Insulin was introduced in 51 GDM patients (45%). In the insulin introduction group, the six-divided diet was less common and the 75-g glucose tolerance test result was positive a significantly greater number of times compared with the non-introduction group. The factor associated with the insulin introduction status was the number of positive 75-g glucose tolerance test results (odds ratio (OR) 2.04, 95% confidence interval (CI): 1.09 - 3.81, P value = 0.025). In addition, the insulin dosage was found to positively correlate with body weight in the non-pregnant state (P value = 0.005).
Conclusions: The six-divided diet was effective for blood glucose control in GDM women. A positive correlation found between the insulin dosage and body weight in the non-pregnant state suggests the importance of proper pre-pregnancy body weight control.
Keywords: Gestational diabetes mellitus; Diet therapy; Insulin therapy; Obesity
| Introduction | ▴Top |
Gestational diabetes mellitus (GDM) can cause fetal hyperglycemia and hyperinsulinemia, resulting in macrosomia or neonatal hypoglycemia [1]. It is also known to be a cause of maternal complications such as pregnancy-induced hypertension and pregnancy wastage [2]. To avoid the risk for these maternal and fetal complications, it is crucial to prevent the onset of GDM or detect and start treatment of GDM at an early stage [3]. After the International Association of Diabetes and Pregnancy Study Group (IADPSG) issued new diagnostic criteria of GDM based on Hyperglycemia and Adverse Pregnancy Outcomes (HAPO) in 2010 [4], the number of GDM patients in Japan has markedly increased compared with that when the conventional criteria were used [5]. The present study aimed to clarify the clinical background, treatment methods (diet therapy and introduction of insulin therapy), and perinatal and postpartum outcomes in GDM patients in our hospital. Predictors of GDM onset and the necessity of insulin treatment identified in this study are expected to contribute to prevent worsening of GDM and maternal and fatal complications through early interventions in GDM as well as provide perinatal care guidance to prevent the onset of GDM; therefore, we believe that this study has an implication for the improvement of maternal and child health.
| Materials and Methods | ▴Top |
This is a retrospective, single-center, observational cohort study. This study was approved by the Ethics Committee of the Jichi Medical University, Saitama Medical Center (No. S17-003) and conforms to the ethical guidelines of the Declaration of Helsinki. In total, 114 pregnant women who underwent GDM screening and were diagnosed with GDM at our hospital between April 2013 and December 2016 were included in this study, except for those with a complication of diabetes mellitus. For GDM screening, a 50-g glucose challenge test (cut-off value: 140 mg/dL) was performed in the second trimester of pregnancy. Women who tested positive in the initial screening test underwent a 75-g oral glucose tolerance test (75-g OGTT), and were diagnosed with GDM if the results meet GDM diagnostic criteria in Guidelines for Obstetrical Practice in Japan 2014 [6].
All women diagnosed with GDM were hospitalized and were fed six-divided diet with tripartition energy (total energy intake (kcal): body mass index (BMI) < 25 kg/m2, standard body weight × 30 + 250 (+ 50 in the first trimester); BMI ≥ 25 kg/m2, standard body weight × 30 according to the Guidelines for the Management of Diabetes Mellitus 2016 [7] under self-monitoring of blood glucose. The target blood glucose level was to satisfy both < 100 mg/dL preprandially and < 120 mg/dL postprandially according to the Guidelines for the Management of Diabetes Mellitus 2016 [7], and the six-divided diet therapy was introduced in the case of poor blood glucose control. Insulin therapy was introduced when the target blood glucose level was not met even after the introduction of the six-divided diet therapy.
Analysis 1: association between the introduction of insulin therapy and background factors in GDM patients
The following background factors were analyzed to check whether they had any association with the introduction of insulin therapy: age (years), prevalence of family history of impaired glucose tolerance, non-pregnant body weight (kg), body weight at delivery (kg), BMI, Apgar scores at 1 min and 5 min (points), newborn weight (g), placental weight (g), introduction of the six-divided diet, the number of positive 75-g OGTT results (positive at one time point vs. positive at two or three time points).
Analysis 2: association between insulin dosage (bolus insulin) and background factors in patients for whom insulin was introduced (51 patients)
The following background factors were analyzed to check whether they had any association with insulin dosage (bolus insulin): age (years), prevalence of family history of impaired glucose tolerance, non-pregnant maternal body weight (kg), placental weight (g), and introduction of the six-divided diet.
Statistical analysis
Results were represented in the form of mean value ± standard deviation or median (25 - 75th percentile). Student’s t-test or U-test was used for comparison between two groups. Fisher’s exact test was used for categorical variables. Multiple regression analysis or logistic regression analysis was used for multivariate analysis. Pearson or Spearman correlation analysis was used for correlation analysis. EZR was used for statistical analyses, and P < 0.05 was considered to indicate a statistically significant difference.
| Results | ▴Top |
In the overall study population, the age was 34.4 ± 4.5 years; insulin was introduced in 51 cases (44.7%) and not introduced in 63 cases; daily insulin dose was 10 ± 15.8 units/day; 48 patients (42.1%) had a family history of impaired glucose tolerance and 66 patients did not; newborn weight was 2,761 ± 446 g; and 66 patients (57.9%) underwent six-divided diet therapy and 48 did not. In 75-g OGTT, 80 patients tested positive once, and 34 patients tested positive two or three times (Table 1).
 Click to view | Table 1. Patient Background |
In analysis 1, background factors with differences between the insulin introduction and non-introduction groups were the introduction of the six-divided diet and number of positive 75-g OGTT results (Table 2). No differences were found with respect to age, prevalence of family history, non-pregnant maternal body weight, prevalence of obesity, newborn weight, or placental weight. In addition, logistic regression analyses were conducted to identify clinical background parameters contributing to the introduction of insulin therapy. Of the explanatory variables (prevalence rates of family history, late-in-life pregnancy, and obesity and the number of positive 75-g OGTT results), the number of positive 75-g OGTT results was the only significant explanatory variable (odds ratio (OR) 2.04, 95% confidence interval (CI): 1.09 - 3.81, P = 0.025) (Table 3).
Click to view | Table 2. Background Factors That Differed Between the Insulin Non-Introduction Group and the Insulin Introduction Group |
Click to view | Table 3. Background Factors Contributing to the Necessity of Insulin Introduction |
In analysis 2, single and multiple regression analyses were performed, and an association was found between insulin dosage and non-pregnant body weight (r = 0.330, P = 0.005) (Table 4). The correlation analysis revealed a positive correlation between the insulin dosage and non-pregnant body weight (r = 0.360, P = 0.012) (Fig. 1). In addition, the insulin dosage was significantly lower in the group of patients who underwent six-divided diet therapy (P = 0.034).
Click to view | Table 4. Insulin Dosage and Background Factors |
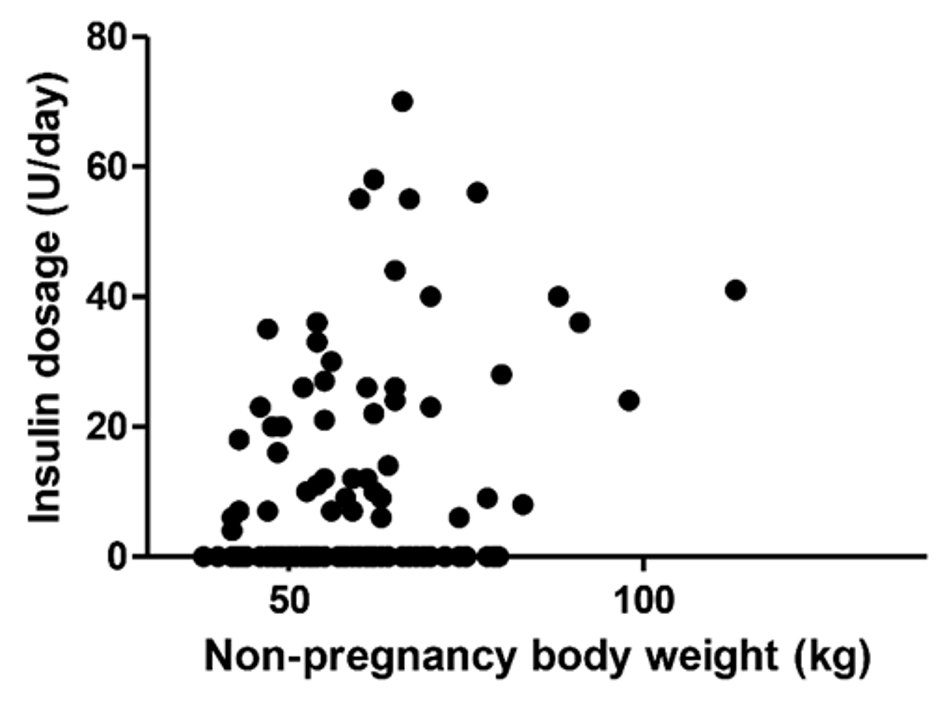 Click for large image | Figure 1. Correlation between non-pregnancy body weight (kg) and insulin dosage (units/day) (r = 0.360, P = 0.012). |
| Discussion | ▴Top |
A previous study has shown that an increased number of positive 75-g OGTT results was associated with an increased likelihood of the introduction of insulin therapy [8]. In analysis 1 of the present study, we explored other factors for determining the introduction of insulin therapy. The first background factor that differed between the insulin introduction and non-introduction groups was the number of positive 75-g OGTT results, as was the case in the previous study. The present study also showed that the necessity of introducing insulin was predictable with the number of positive 75-g OGTT results. Starting therapeutic intervention early in the positive 75-g OGTT result group with obesity, which is a factor requiring insulin treatment identified in a previous study [9], appears to be of particular importance. The presence of obesity was not a risk factor for insulin introduction identified in analysis 1. In Japan, 14.3% of women in their 30s are obese [10]; however, the prevalence of obesity in this study was 38.6%. The higher prevalence is likely because our hospital is a university hospital and has many patients with the obesity complication. A future study with an increased number of patients is necessary.
The second risk for insulin introduction was the six-divided diet; significantly more patients in the insulin introduction group underwent the six-divided diet therapy. In our hospital, patients diagnosed with GDM are hospitalized as a rule, fed with the six-divided diet with tripartition calories according to the Guidelines for the Management of Diabetes Mellitus 2016 [6], and have the blood glucose level measured before and 2 h after each meal. The six-divided diet therapy was introduced if patient’s preprandial and 2-h-postprandial blood glucose levels were ≥ 100 mg/dL and ≥ 120 mg/dL, respectively, for at least 2 days. This is presumably why significantly more patients in the insulin introduction group underwent six-divided diet therapy.
Analysis 2 explored factors related to insulin dosage in the insulin introduction cases. The first factor identified was the introduction of the six-divided diet. The insulin dosage in the six-divided diet introduction group was smaller than that in the non-introduction group. Horie et al have reported that diet therapy improved glucose tolerance and no longer met GDM criteria in the second trimester in 18 of 41 pregnant women who were found to have impaired glucose tolerance in the first trimester [11]. Another study has shown that diet therapy could delay the time of insulin introduction [12]. These findings indicate that the introduction of the six-divided diet is useful for blood glucose control. It is likely that patients with positive 75-g OGTT results benefit from the introduction of diet therapy. In our hospital, nutritionists provide both inpatients and outpatients with nutritional guidance, and pregnant women self-check if the energy intake level is not excessive or deficient with the firm commitment to blood glucose control. Fetal pancreatic β-cells have been reported to be damaged when mother’s energy intake is restricted and can cause impaired glucose tolerance later in life [13]; therefore, it is important that healthcare professionals including physicians, nurses, and nutritionists work together to avoid focusing solely on correcting hyperglycemia and ensure adequate energy intake.
As the second factor, obesity was identified to positively correlate with the insulin dosage. Notably, not the body weight at the time of delivery, but the body weight in the non-pregnant state was a significant positive correlation factor for insulin dosage in this study. Previous studies have shown that mother’s obesity while not pregnant and a history of GDM can be risks for GDM [14, 15] and that normal BMI during non-pregnancy reduces the risk for maternal and fetal complications in GDM [16]. These findings suggest that weight control during non-pregnancy can be a preventive measure against complications, particularly in patients with a history of GDM. It has already been reported that the incidence of type 2 diabetes is high in women with a history of GDM [17]. Therefore, women who wish to get pregnant should be encouraged to learn about the means of preventing obesity, such as diet therapy and exercise therapy, and establish a healthy lifestyle to prevent lifestyle diseases. It has also been reported that children born to pregnant women with the diabetes mellitus complication or to those with GDM develop metabolic syndrome and obesity later in life [18, 19]. Meanwhile, pre-pregnant BMI of < 18.5 kg/m2 has been reported to be associated with an increased risk for low-birth-weight infants [20]. Therefore, to prevent GDM and improve the prognosis of mothers and children, it is important to encourage pre-pregnant women to maintain appropriate body weight.
Acknowledgments
We would like to thank Enago (www.enago.jp) for English language editing.
Financial Disclosure
This work was supported by a Grant-in-Aid for Research Activity start-up (17H07056) to HY from the Japan Society for the Promotion of Science.
Conflict of Interest
The authors declare no conflict of interest.
Informed Consent
Formal informed consent is not required for this retrospective study.
Author Contributions
YM analyzed data and wrote the manuscript; HY conceptualized and drafted the manuscript; MY, DS, RS, MA, SF, IH, KT, and KH collected and analyzed the data.
| References | ▴Top |
- HAPO Study Cooperative Research Group. Hyperglycemia and Adverse Pregnancy Outcome (HAPO) Study: associations with neonatal anthropometrics. Diabetes. 2009;58(2):453-459.
doi pubmed - Temple RC, Aldridge VJ, Murphy HR. Prepregnancy care and pregnancy outcomes in women with type 1 diabetes. Diabetes Care. 2006;29(8):1744-1749.
doi pubmed - American Diabetes Association. 12. Management of diabetes in pregnancy. Diabetes Care. 2016;39(Suppl 1):S94-98.
doi - HAPO Study Cooperative Research Group, Metzger BE, Lowe LP, Dyer AR, Trimble ER, Chaovarindr U, Coustan DR, et al. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med. 2008;358(19):1991-2002.
doi pubmed - Kodama Y, Sameshima H, Ohashi M, Ikenoue T. Impact of new gestational diabetes mellitus criteria on stillbirth: a regional population-based study in Japan. J Obstet Gynaecol Res. 2013;39(7):1242-1245.
doi pubmed - Minakami H, Maeda T, Fujii T, Hamada H, Iitsuka Y, Itakura A, Itoh H, et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J Obstet Gynaecol Res. 2014;40(6):1469-1499.
doi pubmed - Japan Diabetes Society. Guidelines for the management of diabetes mellitus 2016. Tokyo; Nankodo. 2016. (Japanese).
- Ikenoue S, Miyakoshi K, Saisho Y, Sakai K, Kasuga Y, Fukutake M, Izumi Y, et al. Clinical impact of women with gestational diabetes mellitus by the new consensus criteria: two year experience in a single institution in Japan. Endocr J. 2014;61(4):353-358.
doi pubmed - Ouzounian JG, Rosenheck R, Lee RH, Yedigarova L, Walden CL, Korst LM. One-hour post-glucola results and pre-pregnancy body mass index are associated with the need for insulin therapy in women with gestational diabetes. J Matern Fetal Neonatal Med. 2011;24(5):718-722.
doi pubmed - National Health and Nutrition Survey Japan, 2016. http://www.nibiohn.go.jp/eiken/kenkounippon21/en/eiyouchousa/kekka_todoufuken_h28.html.(Japanese). Accessed 5 March 2019.
- Horie I, Kawasaki E, Sakanaka A, Takashima M, Maeyama M, Ando T, Hanada H, et al. Efficacy of nutrition therapy for glucose intolerance in Japanese women diagnosed with gestational diabetes based on IADPSG criteria during early gestation. Diabetes Res Clin Pract. 2015;107(3):400-406.
doi pubmed - Reader D, Splett P, Gunderson EP, Diabetes C, Education Dietetic Practice G. Impact of gestational diabetes mellitus nutrition practice guidelines implemented by registered dietitians on pregnancy outcomes. J Am Diet Assoc. 2006;106(9):1426-1433.
doi pubmed - Fernandez-Twinn DS, Ozanne SE. Mechanisms by which poor early growth programs type-2 diabetes, obesity and the metabolic syndrome. Physiol Behav. 2006;88(3):234-243.
doi pubmed - Black MH, Sacks DA, Xiang AH, Lawrence JM. Clinical outcomes of pregnancies complicated by mild gestational diabetes mellitus differ by combinations of abnormal oral glucose tolerance test values. Diabetes Care. 2010;33(12):2524-2530.
doi pubmed - Sugiyama T, Nagao K, Metoki H, Nishigori H, Saito M, Tokunaga H, Nagase S, et al. Pregnancy outcomes of gestational diabetes mellitus according to pre-gestational BMI in a retrospective multi-institutional study in Japan. Endocr J. 2014;61(4):373-380.
doi pubmed - Rogozinska E, Chamillard M, Hitman GA, Khan KS, Thangaratinam S. Nutritional manipulation for the primary prevention of gestational diabetes mellitus: a meta-analysis of randomised studies. PLoS One. 2015;10(2):e0115526.
doi - Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773-1779.
doi - Barker DJ, Osmond C. Infant mortality, childhood nutrition, and ischaemic heart disease in England and Wales. Lancet. 1986;1(8489):1077-1081.
doi - Moore TR. Fetal exposure to gestational diabetes contributes to subsequent adult metabolic syndrome. Am J Obstet Gynecol. 2010;202(6):643-649.
doi pubmed - Misugi Takuya, et al. The effect of maternal weight gain during pregnancy on prenatal prognosis. Adv Obstet Gynecol. 2013;65(3):243-250.
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.