

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Original Article
Volume 8, Number 7, July 2016, pages 524-530
Hypertension Prevalence, Awareness and Blood Pressure Control in Matao, Brazil: A Pilot Study in Partnership With the Brazilian Family Health Strategy Program
Cesar Minellia, b, d, Lucileni Aparecida Borina, b, Mayra de Cassia Trovob, Geraldo Cassio dos Reisc
aNeurologic Center of Research and Rehabilitation, Matao, SP, Brazil
bHospital Carlos Fernando Malzoni, Matao, SP, Brazil
cDepartment of Neurosciences and Behavioral Sciences, Ribeirao Preto Medical School, University of Sao Paulo, Ribeirao Preto, SP, Brazil
dCorresponding Author: Cesar Minelli, Neurologic Center of Research and Rehabilitation, Rua Sete de Setembro, 568, Centro, Matao, SP 159990-630, Brazil
Manuscript accepted for publication May 10, 2016
Short title: Hypertension Prevalence
doi: http://dx.doi.org/10.14740/jocmr2582w
| Abstract | ▴Top |
Background: Around 30% of Brazilian population is hypertensive. Brazilian’s Family Health Strategy (FHS) is a community-based approach to provide primary health care and control chronic disease as hypertension. The aims of this pilot study were to study hypertension prevalence and awareness and to analyze the feasibility of FHS program with community healthy agents (CHA) to collect data about hypertensive subjects in Matao, Brazil.
Methods: A cross-sectional study was conducted in subjects equal or older than 40 years old in a neighborhood belonging to FHS program. CHA were trained to collect data and to assess blood pressure (BP) with an automated device. Hypertension diagnosis was defined if systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg or subject had previous use of hypertensive drug. Chi-square test and univariate logistic regression analysis were applied with significance level of 5% and a confidence interval of 95%.
Results: In 625 subjects, hypertension prevalence was 68.8% and women (71.9%) were more hypertensive than men (63.2%) (P = 0.02). Prevalence of hypertension increased with age group, from 46.3% (40 - 49 years) to 82.5% (70 - 79 years) (P < 0.001). The overall prevalence of pre-hypertension was 40.1%: stage 1, 25.7% and stage 2, 17.0%. Hypertension awareness was 81.8% and 79.8% reported use of anti-hypertensive drugs. BP was not controlled in 61.8% and 67.7% of them was using anti-hypertensive drugs. CHA reported no difficulties to collect data and BP assessment with the automated device.
Conclusion: We observed a high hypertension prevalence rate, awareness, and subjects with uncontrolled hypertension even with use of anti-hypertensive drugs. CHA from FHS program are a feasible option to BP control in future studies involving larger populations.
Keywords: Hypertension; Epidemiology; Non-communicable diseases; Brazil
| Introduction | ▴Top |
Hypertension is the leading risk factor for death and disability-adjusted life years lost [1]. Most cardiovascular diseases have been attributed to high blood pressure (BP).
In Brazil, hypertension is an important public health problem. Brazilian population-based studies have shown a hypertension prevalence of 35% with a higher rate among men [2]. A systematic review has observed a downward trend in hypertension prevalence from 36.1% in 1980 to 28.7% in 2010, but with different hypertension inclusion criteria between studies [3]. However, other reports have indicated an increase in hypertension prevalence [4-6]. Also, the mortality risk attributed to hypertension was higher among older Brazilian adults compared to an English population with the same demographic aspects [7].
The Family Health Strategy (FHS) program of Brazil is a community-based approach organized by the Ministry of Health to provide primary health care [8]. It consists of teams of doctors, nurses, auxiliary nurses and community health agents (CHA) in predefined areas. One of the main goals of the FHS is to prevent and treat chronic diseases such as hypertension. The participation of CHA in FHS activities is of fundamental importance because these agents are responsible for contacting household members in a geographically delineated micro-area, usually the same micro-area where the agent lives. CHA visit each household within their micro-area at least once a month and collect individual data. Few studies have investigated hypertension in a population covered by the FHS program [9, 10].
The objectives of this pilot study were to determine the prevalence and awareness of hypertension, the use of antihypertensive drugs and the rate of subjects with uncontrolled hypertension in a predefined FHS area and to analyze the feasibility of the FHS program to collect data about hypertensive subjects in Matao, Sao Paulo state, Brazil. We hypothesized that the FHS program with close CHA participation could be an efficient alternative to community BP assessment and control.
| Methods | ▴Top |
Study design
This was a cross-sectional study conducted on all subjects aged 40 years or older. Data about BP, age, gender, previous history of hypertension and use of antihypertensive medication were obtained for all subjects. The exclusion criteria were age of less than 40 years and belonging to another FSH unit.
Characteristics of the city of Matao
The study was performed in Matao, Brazil, a city located in Sao Paulo state, the wealthiest state in Brazil, in the Brazilian southwest, 300 km northwest of the state capital. According to the 2010 Brazilian census, the population of Matao was 76,786 and the estimate for 2015 was 81,439 inhabitants, with no difference in sex distribution [11]. The economy is mainly based on industrial activities and on general services. Ethnicity is diverse, but most people are of Caucasian origin, descendants of European immigrants. The population is urban and stable with a low rate of interurban migration. About 95% of all dwellings have piped water, a sewage network and electricity.
The public health system of Matao is well organized. There are 12 FHS covering a population of 41,400 people, which represents about 50% of the entire population [12]. The study population belongs to FHS “Residencial Cadioli”, which covers 1,454 habitants, with every household and respective residents having been registered. The study was conducted from September to November 2013.
BP assessment
BP was measured by three CHA using the automated device OMRON M2 validated by the European Society of Hypertension [13]. In a 2-h training session, CHA were instructed about the main concepts of hypertension and on how to measure BP properly with the automated device according to the following protocol [14]: BP was measured in both arms; if the readings were different, the arm with the higher reading was used for subsequent measurements 1 - 2 min apart and the average of these measurements was calculated. A wider cuff was used for patients with an arm circumference of more than 32 cm. The patient’s arm being used for the measurement was positioned at the same level as the heart. BP was measured after the patients had emptied their bladders and had abstained from smoking for the last 30 min. The patients sat with their backs supported and with their legs resting on the ground and in the uncrossed position for 5 min.
Outcome variables
One of the following criteria was used for a diagnosis of hypertension [14]: systolic blood pressure (SBP) ≥ 140 mm Hg or diastolic blood pressure (DBP) ≥ 90 mm Hg or use of hypertensive medication. Hypertension was classified as pre-hypertension if SBP was between 120 and 139 mm Hg or DBP was between 80 and 89 mm Hg, as stage 1 hypertension if SBP was 140 - 159 mm Hg or DBP was 90 - 99 mm Hg, and as stage 2 hypertension if SBP was ≥ 160 mm Hg or DBP was ≥ 100 mm Hg. Hypertension awareness was defined if the subject had previous knowledge of a diagnosis of hypertension. Use of antihypertensive medication was defined if the patients said that they were taking drugs to control their BP.
Statistical analysis
Qualitative variables were presented as absolute and relative frequency, and quantitative variables as mean and standard deviation. Associations between the prevalence and awareness of hypertension and the variables “sex” and “age” were analyzed by the Chi-square test. Univariate logistic regression analysis was carried out using hypertension as the dependent variable and age as the independent variable. Analyses were performed using SPSS software version 17. For all tests, we considered a level of significance of 5% and a 95% confidence interval (CI).
Ethics
The research project number 296.915 was evaluated and approved by the Institutional Ethics Committee of Centro Universitario Barao de Maua, and all participants and CHA gave written informed consent to participate.
| Results | ▴Top |
The initial sample consisted of 1,454 participants. Of these, 829 were excluded for the following reasons: 690 were not found during a home visit, 109 had incomplete data, 21 refused BP assessment, four had moved to another address, and five had died. Therefore, the final sample consisted of 625 subjects (mean age: 62.6 ± 12.5 years) (Fig. 1). Of these, 64.8% were females. Mean SBP was 138.1 ± 22.6 mm Hg and DBP was 79.0 ± 12.6 mm Hg.
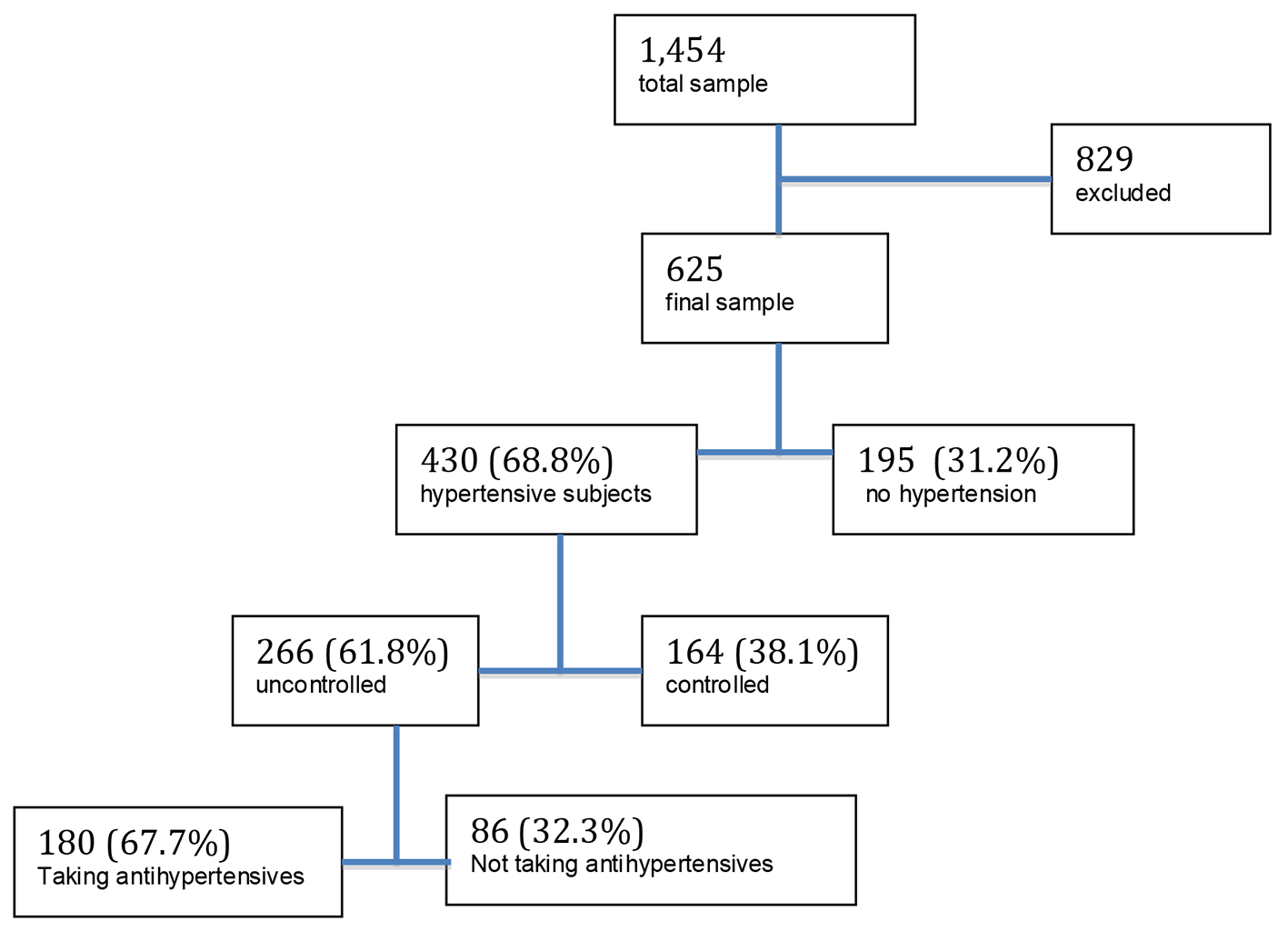 Click for large image | Figure 1. Sample selection. |
The prevalence of hypertension was 68.8% (430/625), was higher among women (71.9%) than men (63.2%) (P = 0.02) and increased with age group from 46.3% (40 - 49 years) to 82.5% (70 - 79 years), followed by a significant 5% reduction, i.e., 77.6% among subjects older than 80 years (P < 0.001). The chance of hypertension increased by 54% in each 10 years age group (odds ratio (OR): 1.54; 95% CI: 1.33 - 1.80) and by 5% in each year (OR: 1.05; 95% CI: 1.03 - 1.06) (Table 1).
 Click to view | Table 1. Hypertension Status According to Gender and Age Group |
Regarding the classification of hypertension, the overall prevalence of pre-hypertension was 40.1%; the prevalence of stage 1 was 25.7% and the prevalence of stage 2 was 17.0%. In the age groups of 40 - 49 to 70 - 79 years, the prevalence of pre-hypertension stages was higher for younger ages and declined with advanced age. The opposite occurred with hypertension stages 1 and 2, with low rates among younger subjects and a progressive increase among older subjects, with hypertension stage 2 reaching a prevalence of 28.2% in the 70 - 79 year age group (P < 0.001) (Fig. 2). These tendencies were not so evident in the ≥ 80 age group. There was no difference in hypertension stages between gender (P = 0.17) (Fig. 3).
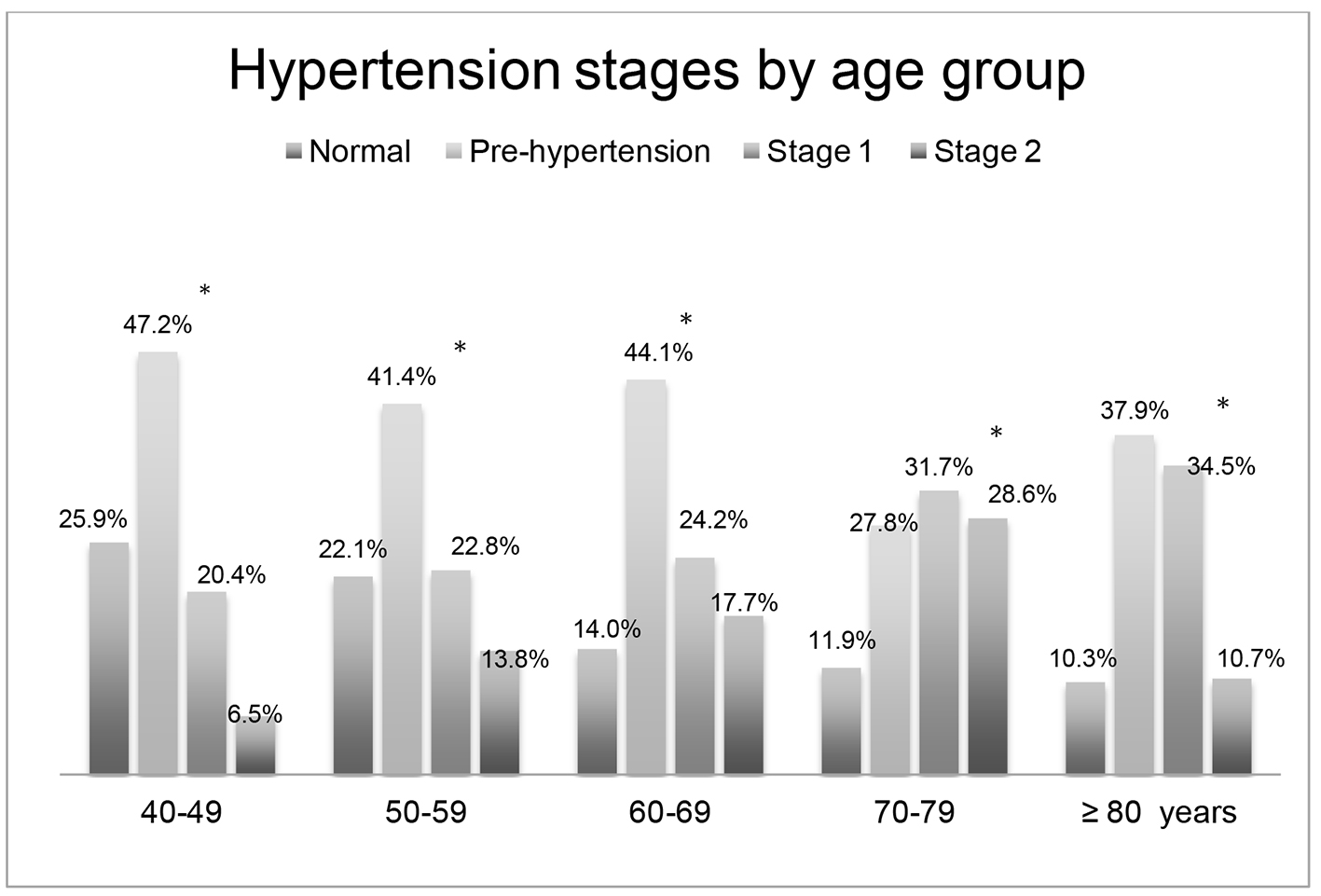 Click for large image | Figure 2. Hypertension stages by age group. *There were significant differences in hypertension stages between age groups (P < 0.001). |
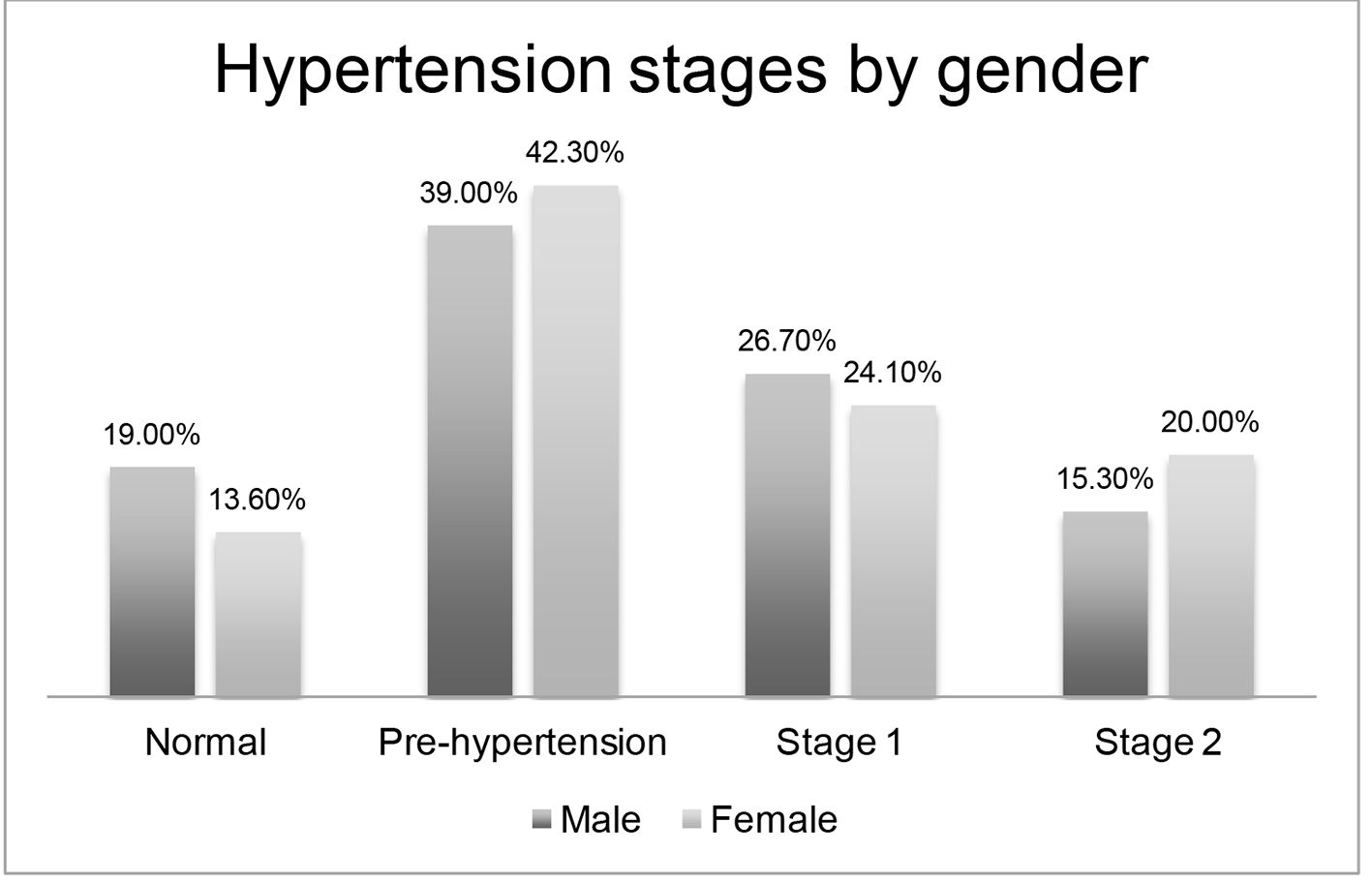 Click for large image | Figure 3. Hypertension classification by gender. There was no difference in hypertension stages or gender (P = 0.17). |
Of 430 hypertensive subjects, 352 (81.8%) were aware of their hypertension and 343 (79.8%) reported the use of antihypertensive drugs. Hypertension awareness and use of antihypertensive drugs were more prevalent among women (P < 0.001) (Table 2). Awareness and use of antihypertensive drugs were more prevalent among subjects with normal and pre-hypertension stages than among subjects with stage 1 and 2 hypertension. There was no difference between age groups regarding awareness or use of antihypertensive drugs.
Click to view | Table 2. Hypertension Awareness and Use of Antihypertensive Drugs According to Gender, Age Group and Hypertension Stage |
BP was uncontrolled in 266 (61.8 %) of 430 hypertensive subjects. Of the 266 subjects with uncontrolled hypertension, 180 (67.7%) said that they were using antihypertensive medication.
The limitation reported by CHA was the distance from some houses. There were no difficulties in BP assessment with the automated device and CHA reported that the method was practical and easy to use.
| Discussion | ▴Top |
This pilot study conducted in Matao demonstrated one of highest rates of hypertension among the rates reported for Brazil [15-24]. The partnership with the FHS program using CHA for BP assessment and demographic data collection was practical and reliable, involving a method easy to apply.
Some reasons can explain the high hypertension prevalence observed in the present study. Our population was older (≥ 40 years) compared to other studies that included subjects ≥ 18 years old. Also, BP was assessed only once and may have overestimated the prevalence of hypertension. Recent hypertension guidelines have recommended a second BP measurement to confirm a diagnosis of hypertension [14, 25].
The present data show that women were more hypertensive than men, an opposite result compared to that reported in a recent review [2]. Almost half the subjects in the initial sample were not found on the occasion of the home visit by CHA because they were at work and most of these subjects were men. Thus, this sample bias may have contributed to the significant prevalence of hypertension among women.
The latest Brazilian population studies about hypertension awareness, use of antihypertensive drugs and subjects with controlled BP have reported rates ranging from 44.1% to 81.5%, 36.3% to 85.4% and 22.0% to 60.1% [26-30]. This wide variation in rates can be justified by differences in age groups, socioeconomic conditions and methodological analysis among studies. Our study showed a high percentage of hypertension awareness and of subjects using antihypertensive drugs, which are close to rates reported for Catanduva [26], a city close to Matao. Since these cities are located in one of the wealthiest regions in Brazil, a better knowledge of hypertension and the importance of the use of antihypertensive drugs emphasized in extensive public campaigns could explain these numbers. The higher prevalence of hypertension awareness and use of antihypertensive drugs in women have also been observed in other studies [24, 27, 28, 30].
However, in line with other studies [16, 17, 20, 21], almost two-thirds of our subjects had uncontrolled hypertension. As a paradox, even with a high level of awareness and use of antihypertensive drugs, 61.8% of our subjects had uncontrolled BP. Since 67.7% of these uncontrolled subjects said that they were using antihypertensive drugs, we may assume that treatment is failing probably because of at least one of the following reasons: low adherence to follow-up, insufficient dose of antihypertensive drugs or necessity to add other antihypertensive drugs. Many subjects believe that only using antihypertensive drugs, without regular BP assessment is enough for BP control [31].
Our results showed that almost half the subjects in the 40 - 49 year age group had pre-hypertension and almost one-third of subjects in the 70 - 79 year age group had stage 2 hypertension. Advanced age has been already recognized as a risk factor associated with increase hypertension prevalence [32, 33]. It is fundamental to identify these groups at higher risk to develop hypertension and cardiovascular disease in order to implement lifestyle modifications and to improve pharmacological treatment [34].
Our study has some limitations. A sample bias occurred because more than half subjects in the initial sample were away at work on the occasion of the CHA home visit and were not included. Future studies will require a schedule home visit to find some subjects. All patients were evaluated in the morning due to the time scheduled for the CHA’s home visit. Subjects with masked hypertension with poor BP control at night could not have been identified. Subjects younger than 40 years were not included in our sample. The hypertension prevalence might have been lower if adults 18 - 39 years old had been included. The reason to include subjects older than 40 was justified by the fact that almost 20% of subjects aged 35 - 44 years already have hypertension according to the Brazilian Ministry of Healthy [35]. Moreover, our research group is preparing a larger study for hypertension prevention and pharmacological treatment focusing on subjects older than 40 years.
The more positive aspect of this study was the feasibility of hypertension data collected by CHA. Previous studies have suggested that community interventions including BP monitoring in a non-clinical setting and using community resources show promising results in terms of reducing and controlling BP among hypertensive patients [36, 37]. Also, since CHA are members of the FHS program, no additional cost was necessary regarding human resources. The only additional costs involved the acquisition of three automated devices for BP measurement bought for U$59.40 each. Although CHA reported that distance was a problem for some houses, this could be overcome in future studies using alternatives means of transportation.
Therefore, this pilot study can serve as a base to support a larger study involving other neighborhoods in Matao and also as a model of BP control to be implemented in cities with the same health system characteristics.
Conclusions
We observed a high prevalence of hypertension, awareness, use of antihypertensive medication and many subjects with uncontrolled hypertension. Women were more hypertensive than men and advanced age was associated with a higher prevalence of hypertension. Also, almost two-thirds of the subjects were using antihypertensive drugs and most of them had uncontrolled BP. Our study confirmed that target blood pressure levels are seldom achieved in a large proportion of hypertensive subjects regardless of whether treatment is prescribed or not. Moreover, CHA were a convenient alternative to BP assessment in a large population. The identification of populations at higher risk to develop hypertension and cardiovascular disease is fundamental to direct public health strategies.
| References | ▴Top |
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224-2260.
doi - Ribeiro AL, Duncan BB, Brant LC, Lotufo PA, Mill JG, Barreto SM. Cardiovascular Health in Brazil: Trends and Perspectives. Circulation. 2016;133(4):422-433.
doi pubmed - Picon RV, Fuchs FD, Moreira LB, Riegel G, Fuchs SC. Trends in prevalence of hypertension in Brazil: a systematic review with meta-analysis. PLoS One. 2012;7(10):e48255.
doi pubmed - Gus I, Ribeiro RA, Kato S, Bastos J, Medina C, Zazlavsky C, Portal VL, et al. Variations in the Prevalence of Risk Factors for Coronary Artery Disease in Rio Grande do Sul-Brazil: A Comparative Analysis between 2002 and 2014. Arq Bras Cardiol. 2015;105(6):573-579.
doi - Ferreira HS, Lucio GM, Assuncao ML, Silva BC, Oliveira JS, Florencio TM, Geraldes AA, et al. High Blood Pressure among Students in Public and Private Schools in Maceio, Brazil. PLoS One. 2015;10(11):e0142982.
doi pubmed - Nascimento Cde M, Mambrini JV, de Oliveira CM, Giacomin KC, Peixoto SV. Diabetes, hypertension and mobility among Brazilian older adults: findings from the Brazilian National Household Sample Survey (1998, 2003 and 2008). BMC Public Health. 2015;15:591.
doi pubmed - de Oliveira C, Marmot MG, Demakakos P, Vaz de Melo Mambrini J, Peixoto SV, Lima-Costa MF. Mortality risk attributable to smoking, hypertension and diabetes among English and Brazilian older adults (The ELSA and Bambui cohort ageing studies). Eur J Public Health. 2015.
doi pubmed - Macinko J, Harris MJ. Brazil's family health strategy--delivering community-based primary care in a universal health system. N Engl J Med. 2015;372(23):2177-2181.
doi pubmed - de Paula JA, Moreira OC, da Silva CD, Silva DS, dos Santos Amorim PR. Metabolic syndrome prevalence in elderly of urban and rural communities participants in the HIPERDIA in the city of Coimbra/MG, Brazil. Invest Educ Enferm. 2015;33(2):325-333.
pubmed - Cotta RM, Batista KC, Reis RS, de Souza GA, Dias G, de Castro FA, Alfenas Rde C. [Social-sanitary and lifestyle profile of hypertense and/or diabetics, users of the Family Health Program in the city of Teixeiras, Minas Gerais State]. Cien Saude Colet. 2009;14(4):1251-1260.
doi pubmed - Instituto Brasileiro de Estatististica e Geografia. Censo 2010. http://cidades.ibge.gov.br/xtras/perfil.php?lang=&codmun=352930. Acessed in March 6, 2016.
- Ministerio da Saude. DATASUS. http://dab.saude.gov.br/portaldab /historico_ cobertura_sf.php/Unidade Geografica/Sao Paulo/Matao/Periodo 2015. Acessed December 15, 2015
pubmed - Topouchian J, Agnoletti D, Blacher J, Youssef A, Ibanez I, Khabouth J, Khawaja S, et al. Validation of four automatic devices for self-measurement of blood pressure according to the international protocol of the European Society of Hypertension. Vasc Health Risk Manag. 2011;7:709-717.
pubmed - Weber MA, Schiffrin EL, White WB, Mann S, Lindholm LH, Kenerson JG, Flack JM, et al. Clinical practice guidelines for the management of hypertension in the community a statement by the American Society of Hypertension and the International Society of Hypertension. J Hypertens. 2014;32(1):3-15.
doi pubmed - da Costa JS, Barcellos FC, Sclowitz ML, Sclowitz IK, Castanheira M, Olinto MT, Menezes AM, et al. Hypertension prevalence and its associated risk factors in adults: a population-based study in Pelotas. Arq Bras Cardiol. 2007;88(1):59-65.
pubmed - Castro RA, Moncau JE, Marcopito LF. Hypertension prevalence in the city of Formiga, MG, Brazil. Arq Bras Cardiol. 2007;88(3):334-339.
doi pubmed - Jardim PC, Gondim Mdo R, Monego ET, Moreira HG, Vitorino PV, Souza WK, Scala LC. High blood pressure and some risk factors in a Brazilian capital. Arq Bras Cardiol. 2007;88(4):452-457.
doi pubmed - Barbosa JB, Silva AA, Santos AM, Monteiro Junior F, Barbosa MM, Figueiredo Neto JA, Soares Nde J, et al. Prevalence of arterial hypertension and associated factors in adults in Sao Luis, state of Maranhao. Arq Bras Cardiol. 2008;91(4):236-242, 260-236.
- Barbosa LS, Scala LN, Ferreira MG. Associacao entre marcadores antoprometricos de obesidade central e hipertensao arterial na populacao adulta de Cuiaba, Mato Gorsso. Rev Bras Epidemiol. 2009;12:237-247.
doi - Longo GZ, Neves J, Luciano VM, Peres MA. Prevalence of high blood pressure levels and associated factors among adults in Southern Brazil. Arq Bras Cardiol. 2009;93(4):387-394, 380-386.
- Rosario TM, Scala LC, Franca GV, Pereira MR, Jardim PC. Fatores associados a hipertensao arterial sistemica em Nobres-MT. Rev Bras Epidemiol. 2009;12:248-257.
doi - Nascente FM, Jardim PC, Peixoto Mdo R, Monego ET, Moreira HG, Vitorino PV, Souza WK, et al. [Arterial hypertension and its correlation with some risk factors in a small brazilian town]. Arq Bras Cardiol. 2010;95(4):502-508.
doi pubmed - Unger A, Felzemburgh RD, Snyder RE, Ribeiro GS, Mohr S, Costa VB, Melendez AX, et al. Hypertension in a Brazilian urban slum population. J Urban Health. 2015;92(3):446-459.
doi pubmed - Doulougou B, Gomez F, Alvarado B, Guerra RO, Ylli A, Guralnik J, Zunzunegui MV. Factors associated with hypertension prevalence, awareness, treatment and control among participants in the International Mobility in Aging Study (IMIAS). J Hum Hypertens. 2016;30(2):112-119.
doi pubmed - Daskalopoulou SS, Rabi DM, Zarnke KB, Dasgupta K, Nerenberg K, Cloutier L, Gelfer M, et al. The 2015 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention, and treatment of hypertension. Can J Cardiol. 2015;31(5):549-568.
doi pubmed - Freitas OC, Resende de Carvalho F, Marques Neves J, Veludo PK, Silva Parreira R, Marafiotti Goncalves R, Arenales de Lima S, et al. Prevalence of hypertension in the urban population of Catanduva, in the State of Sao Paulo, Brazil. Arq Bras Cardiol. 2001;77(1):9-21.
doi pubmed - Jardim T, Neiva T, Rodrigues R, Arantes A, Barros C, Chinem B, Rocha R, et al. 5c.05: Differences in Prevalence, Awareness, Treatment and Control Rates of Hypertension between Male and Female. J Hypertens. 2015;33(Suppl 1):69e.
doi pubmed - Nogueira D, Faerstein E, Coeli CM, Chor D, Lopes Cde S, Werneck GL. [Awareness, treatment, and control of arterial hypertension: Pro-Saude study, Brazil]. Rev Panam Salud Publica. 2010;27(2):103-109.
doi pubmed - Almeida RC, Dias DJ, Deguchi KT, Spesia CH, Coelho OR. Prevalence and treatment of hypertension in urban and riverside areas in Porto Velho, the Brazilian Amazon. Postgrad Med. 2015;127(1):66-72.
doi pubmed - Pereira MR, Coutinho MS, Freitas PF, D'Orsi E, Bernardi A, Hass R. [Prevalence, awareness, treatment, and control of hypertension in the adult urban population of Tubarao, Santa Catarina, Brazil, 2003]. Cad Saude Publica. 2007;23(10):2363-2374.
doi pubmed - Arima H, Barzi F, Chalmers J. Mortality patterns in hypertension. J Hypertens. 2011;29(Suppl 1):S3-7.
doi pubmed - Vasan RS, Beiser A, Seshadri S, Larson MG, Kannel WB, D'Agostino RB, Levy D. Residual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart Study. JAMA. 2002;287(8):1003-1010.
doi pubmed - Bromfield SG, Bowling CB, Tanner RM, Peralta CA, Odden MC, Oparil S, Muntner P. Trends in hypertension prevalence, awareness, treatment, and control among US adults 80 years and older, 1988-2010. J Clin Hypertens (Greenwich). 2014;16(4):270-276.
doi pubmed - Poulter NR, Prabhakaran D, Caulfield M. Hypertension. Lancet. 2015;386(9995):801-812.
doi - Ministerio da Saude. DATASUS. http://tabnet.datasus.gov.br/cgi/tabnet.exe?idb2012/g02.def. Assessed December 16, 2015.
- Jones C, Simpson SH, Mitchell D, Haggarty S, Campbell N, Then K, Lewanczuk RZ, et al. Enhancing hypertension awareness and management in the elderly: lessons learned from the Airdrie Community Hypertension Awareness and Management Program (A-CHAMP). Can J Cardiol. 2008;24(7):561-567.
doi - Kaczorowski J, Chambers LW, Dolovich L, Paterson JM, Karwalajtys T, Gierman T, Farrell B, et al. Improving cardiovascular health at population level: 39 community cluster randomised trial of Cardiovascular Health Awareness Program (CHAP). BMJ. 2011;342:d442.
doi pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.