

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Letter to the Editor
Volume 8, Number 2, February 2016, pages 178-179
Interhemispheric Acute Subdural Hematoma: A Distinct Entity of Subdural Hematoma
Ozgur Soguta, f, Mehmet Yigita, Kenan Ahmet Turkdoganb, Eda Yigitc, Bedia Gulend, Ertan Sonmezd, Onur Kaplana, Huseyin Toprake
aDepartment of Emergency Medicine, Haseki Training and Research Hospital, Istanbul, Turkey
bDepartment of Emergency Medicine, School of Medicine, Aydin Menderes University, Aydin, Turkey
cDepartment of Emergency Medicine, Sisli Etfal Training and Research Hospital, Istanbul, Turkey
dDepartment of Emergency Medicine, School of Medicine, Bezmialem Vakif University, Istanbul, Turkey
eDepartment of Radiology, School of Medicine, Bezmialem Vakif University, Istanbul, Turkey
fCorresponding Author: Ozgur Sogut, Department of Emergency Medicine, Haseki Training and Research Hospital, Istanbul, Turkey
Manuscript accepted for publication December 11, 2015
Short title: Interhemispheric Acute Subdural Hematoma
doi: http://dx.doi.org/10.14740/jocmr2427w
| To the Editor | ▴Top |
We wish to notify the readers on a rare case of interhemispheric acute subdural hematoma (ASH) who presented to our emergency department (ED) with a falx syndrome of contralateral hemiparesis in lower extremity and severe headache. A 25-year-old previously healthy man was involved in a traffic accident and presented to our ED with complaints of repeated vomiting and severe headache. On arrival to the ED, he had an initial Glasgow coma scale (GCS) of 14 (opening her eyes with verbal stimuli, obeys commands, orientated) and normal vital signs (blood pressure: 130/85 mm Hg; heart rate: 86 bpm). No other injuries were noted. Neurological examination revealed mild weakness of the right lower extremity (strength score: 4/5). His routine blood tests, including complete blood counts, prothrombin time, and thromboplastin time were unremarkable. The plain films of the skull were normal. Non-enhanced cranial (CT) scan performed 4 h after the accident revealed a small left-sided acute interhemispheric subdural hematoma, which was posteriorly located (Fig. 1a). Magnetic resonance imaging (MRI) of the brain during the first 24 h after admission confirmed minimal ASH in the posterior interhemispheric fissure with subacute subdural hematoma in the left parieto-occipital cortex and occipital regions (Fig. 1b). Considering the clinical condition of the patient, surgery was not planned by the neurosurgical department but the patient was kept under observation in the ED. He was discharged home 48 h after the trauma with a normal neurological examination and mild intermittent headaches.
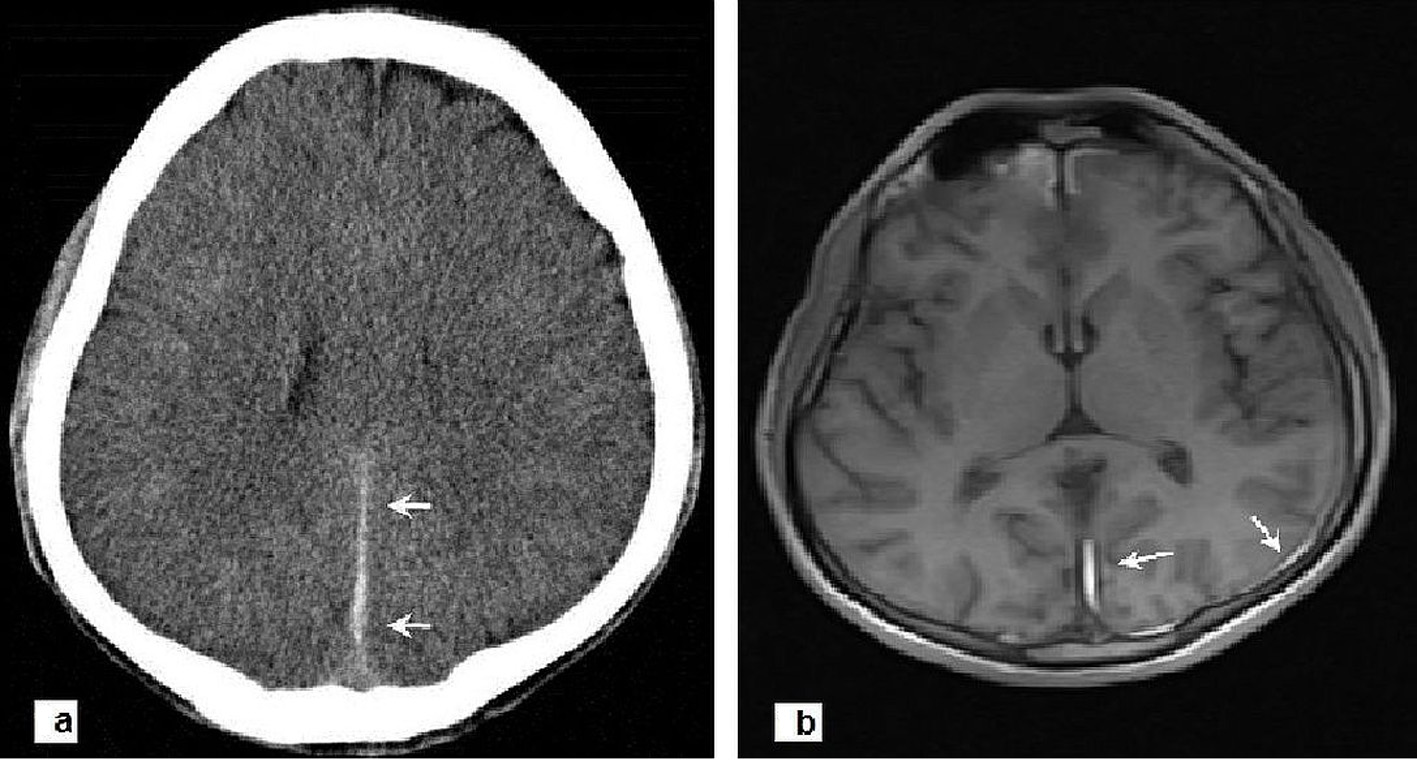 Click for large image | Figure 1. (a) Axial CT scan of brain performed 4 h after the accident revealing a small left-sided acute interhemispheric subdural hematoma, which was posteriorly located (arrows). (b) Cranial MRI showing minimal ASH in the posterior interhemispheric fissure (arrows) with subacute subdural hematoma in the left parieto-occipital cortex and occipital regions (arrows). |
Interhemispheric ASH is a relatively uncommon type of ASH because of their unusual location [1]. They usually occur in patients with bleeding disorders and are associated with trauma in the majority of cases [2]. Computed tomography (CT) and MRI are important neuroradiological techniques for the accurate diagnosis of interhemispheric ASH [1, 2]. Although interhemispheric ASH is a rare form of subdural hematoma, early diagnosis and treatment is of great importance because of its emergent condition [2, 3]. CT and MRI are important diagnostic tools, as it was in this case. MRI may have the advantage rather than CT due to the absence of beam-hardening and multiplanar imaging. The best management modality for interhemispheric ASH depends upon the neurologic status on admission and clinical course [2]. If the patient is neurologically stable, conservative treatment is generally preferred. Surgical treatment is reserved in patients with disturbances of consciousness and for patients with progressive neurological deterioration [3].
| References | ▴Top |
- Shankar A, Joseph M, Chandy MJ. Interhemispheric subdural hematoma: an uncommon sequel of trauma. Neurol India. 2003;51(1):63-64.
pubmed - Carangelo B, Peri G, Palma L. Post-traumatic interemispheric subdural hematoma: report of two cases and review of the literature. J Neurosurg Sci. 2011;55(1):81-84.
pubmed - Kawoosa NN, Bhat AR, Rashid B. Interhemispheric acute subdural hematomas. Iran Red Crescent Med J. 2011;13(4):289-290.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.