

| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 1, Number 4, October 2009, pages 240-243
Doppler Echocardiographic Diagnosis of a Rare Pentalogy of Fallot Having Penta-Cardiac Anomalies: A Case Report
Mohd Suhaila, b, c, Mohd Faizul-Suhailb, Hina Khanb, Safia Suhailb
aDepartment of Biochemistry, University of Allahabad, Allahabad-211002, India
bCity Nursing & Maternity Home Research Center, 21, Minhajpur, Allahabad-211003, India
cCorresponding author:
Manuscript accepted for publication September 09, 2009
Short title: Pentalogy of Fallot
doi: https://doi.org/10.4021/jocmr2009.09.1261
| Abstract | ▴Top |
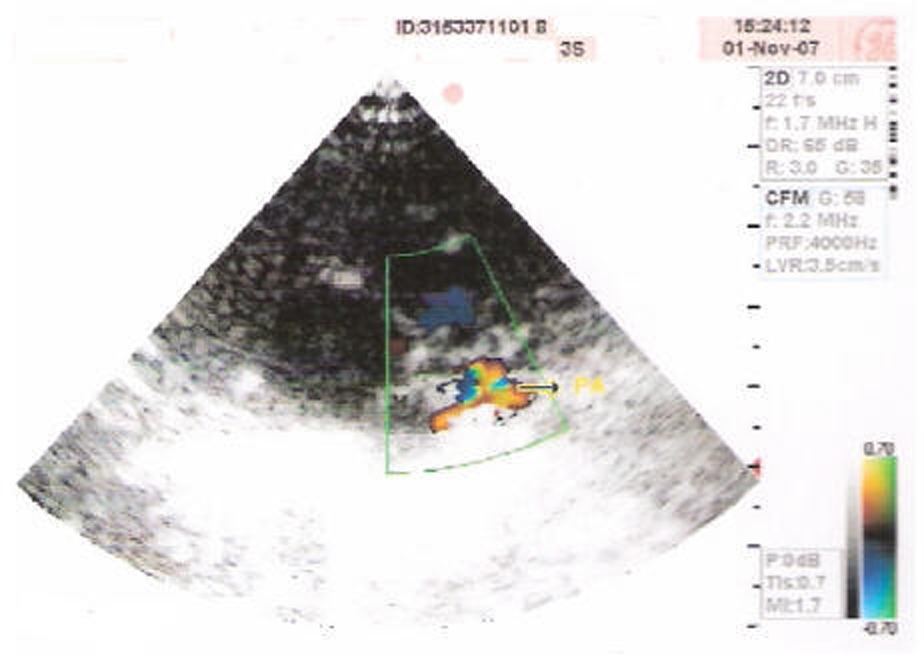
An infant, showing peripheral cyanosis, was born after lower abdominal peripheral caesarian section of the pregnant women having TORCH positive test with the infection of Toxoplasma gondiiand Cytomegalovirus. She had three abortions prior to this pregnancy. Doppler echocardiography of the baby showed profound intracardiac defects. After birth, echocardiography was carried out for diagnosis of associated cardiac anomalies. Doppler echocardiography showed pentalogy of Fallot, and the present case represents the Pentalogy of Fallot having pulmonary atresia. The baby's heart anomalies were ASD (Atrial Septal Defect - 6 mm RT to LT Shunt), VSD (Ventricular Septal Defect - bidirectional shunt), PDA (Patent Ductus Arteriosus - filling both the pulmonary arteries), and Overriding of Aorta with pulmonary atresia. In conclusion, whenever the diagnosis pentalogy of fallot is suspected, a multidisciplinary approach is essential.
Keywords: Pentalogy of fallot; Overriding Aorta; Ventricular Septal Defect; Atrial Septal Defect; Pulmonary Atresia; Doppler Echocardiography
| Introduction | ▴Top |
Tetralogy of Fallot [1], also known as Fallot's syndrome or Fallots tetrad, has four key features. A ventricular septal defect (a hole between the ventricles) and many levels of obstruction from the right ventricle to the lungs (pulmonary stenosis) are the most important. Also, the aorta (major artery from the heart to the body) lies directly over the ventricular septal defect, and the right ventricle develops thickened muscle. Because the aorta overrides the ventricular defect and there's pulmonary stenosis, blood from both ventricles (oxygen-rich and oxygen-poor) is pumped into the body. Sometimes the pulmonary valve is completely obstructed (pulmonary atresia). Infants and young children with unrepaired tetralogy of Fallot are often blue (cyanotic) as in the present case. The reason is that some oxygen-poor blood is pumped to the body.
| Case Report | ▴Top |
A 2.5 kg infant was born at 38 weeks gestation after lower abdominal caesarian section (L.A.C.S.) of 25 years old woman having breech presentation in our hospital. The female child showed peripheral cyanosis as evident from the Figure 1.
 Click for large image | Figure 1. Showing peripheral cyanosis over a palm. |
The association of tetralogy of Fallot with anomalous pulmonary venous drainage is rare and only limited number of cases have been reported till now [2,3]. It is estimated that 8% of cardiac malformations are due to genetic factors, 2% to environmental agents, and the vast majority to a complex interplay between genetic and environmental influences [4]. Classic examples of environmental cardiovascular teratogens include rubella virus. In the present case, the mother giving birth to the newborn was having infection of rubella virus as well.
Mostly, the defect is due to antero-cephalad deviation of the outlet septum resulting in: (i) an unrestricted large anterior malalignment subaortic VSD; (ii) right ventricular outflow tract obstruction which may be infundibular valvular, supravalvular or a combination of all; (iii) consequent right ventricular hypertrophy; and (iv) an overriding aorta (< 50%). Accompanying features can include additional muscular VSDs, anomalous coronary arteries, a right-sided aortic arch, PDA, aortic root dilation, and aortopulmonary collaterals (mainly seen in patients with pulmonary atresia / VSD). Use of prenatal magnetic resonance imaging (MRI) may enhance the visualization of the fetal anomalies [5]. After birth, echocardiography is essential for diagnosis of associated cardiac anomalies.
Nevertheless, small defects of the diaphragm and pericardium can be extremely difficult to diagnose accurately. In these patients and in cases of possible surgical intervention, MRI might be useful [6,7]. MRI provides good delineation of the aorta, right ventricular outflow tract, VSDs, right ventricular hypertrophy, and the pulmonary artery and its branches. MRI can be used to measure intracardiac pressures, gradients, and blood flows. The treatment of the pentalogy of Fallot consists ofcorrective cardiovascular surgery. However, in the present case the mother and her attendants were advised to go for the cardiovascular surgery, but before they could decide, the child expired.
In conclusion, careful preoperative assessment is required in those with totally anomalous connections. Whenever, the diagnosis of pentalogy of Fallot is suspected, a multidisciplinary approach is essential. A prenatal medical team consisting of a gynecologist, a neonatologist, a pediatric cardiologist, a geneticist, and a pediatric surgeon should use their expertise in choosing the best approach to this severe disorder.
Competing Interests
The authors declare no conflict of interest.
| References | ▴Top |
- E. L. A. Fallot. Contribution à l'anatomie pathologique de la maladie bleue (cyanose cardiaque). Marseille médical. 1888;25:77-93, 138-158, 207-223, 341-354, 370-386, 403-420.
- Gerlis LM, Fiddler GI, Pearse RG. Total anomalous pulmonary venous drainage associated with tetralogy of Fallot: report of a case. Pediatr Cardiol. 1983;4(4):297-299.
pubmed - Gutierrez J, Perez de Leon J, de Marco E, Gomez R, Cazzaniga M, Vellibre D, Quero Jimenez M,
et al . Tetralogy of Fallot associated with total anomalous pulmonary venous drainage. Pediatr Cardiol. 1983;4(4):293-295. - Pierpont MEM, Moller JH. Genetics of Cardiovascular Disease. Boston, Martinus Nijhoff. 1987;
- McMahon CJ, Taylor MD, Cassady CI, Olutoye OO, Bezold LI. Diagnosis of pentalogy of cantrell in the fetus using magnetic resonance imaging and ultrasound. Pediatr Cardiol. 2007;(3):172(175):
pubmed - Oka T, Shiraishi I, Iwasaki N, Itoi T, Hamaoka K. Usefulness of helical CT angiography and MRI in the diagnosis and treatment of pentalogy of Cantrell. J Pediatr. 2003;142(1):
pubmed - Song A, McLeary MS. MR imaging of pentalogy of Cantrell variant with an intact diaphragm and pericardium. Pediatr Radiol. 2000;30(9):638-639.
pubmed
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.