Figures
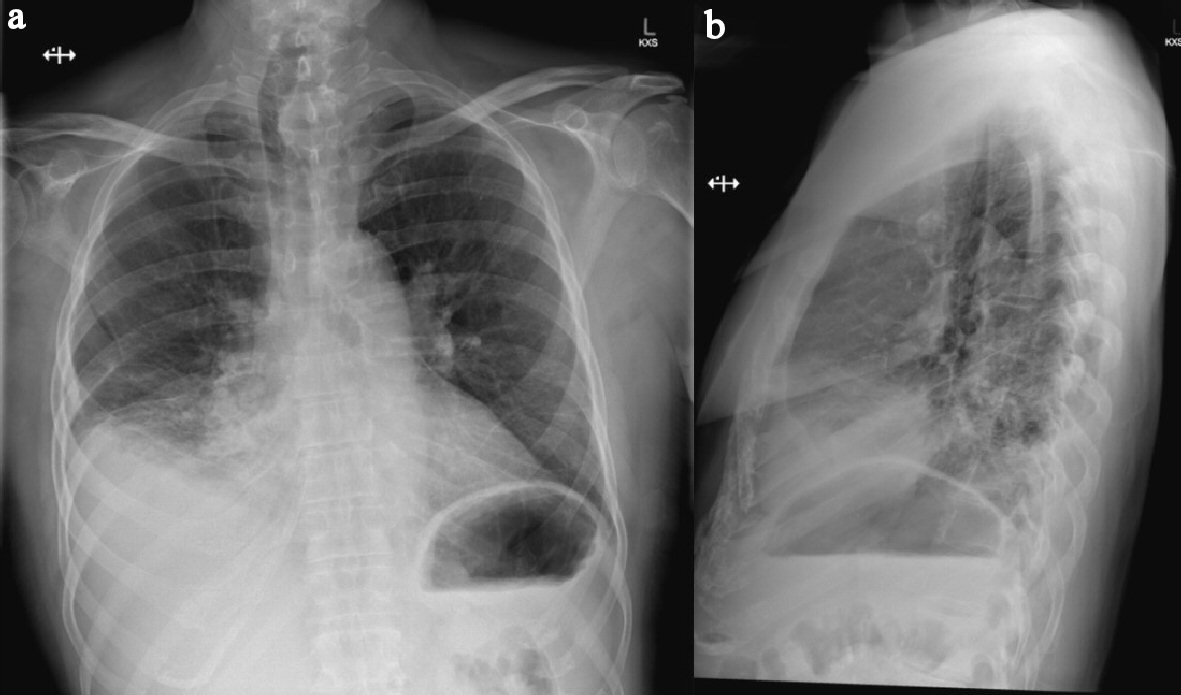
Figure 1. (a) Erect PA chest X-ray showing consolidation and atelectatic changes of right middle and lower lobes obscuring hemidiaphragm with associated mild effusion. (b) Lateral view of same chest X-ray. Note: trachea displaced to the right consistent with known left retrosternal thyroid goitre.
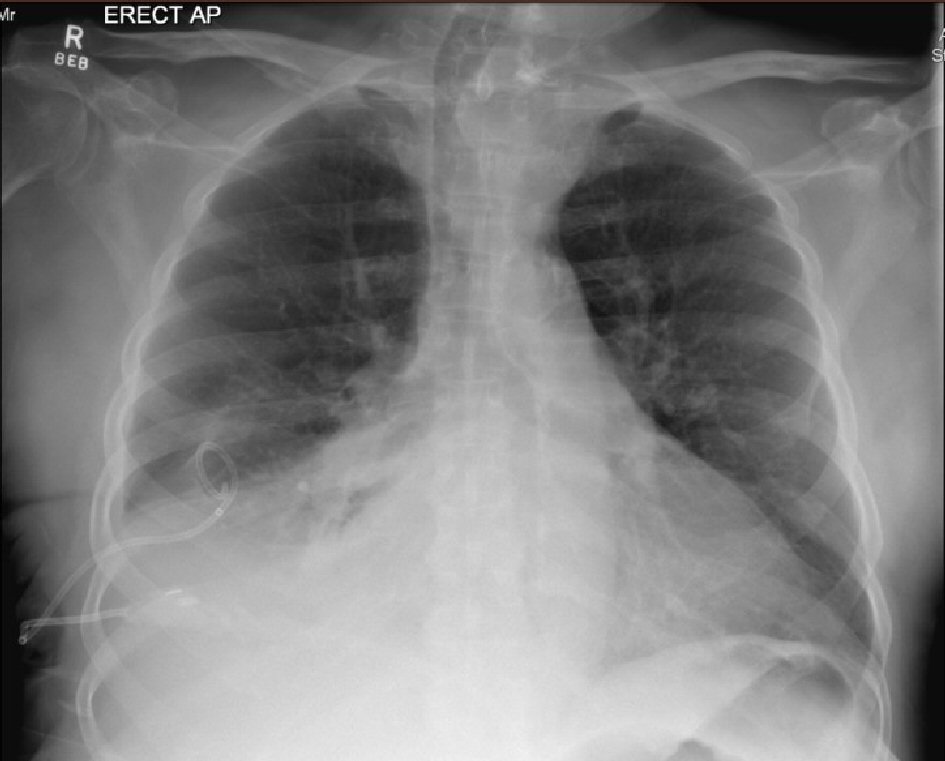
Figure 2. Erect AP chest X-ray showing newly inserted right-sided chest drain in situ, collapse of right lung base and moderate resolution of right-sided pleural effusion. Remaining lungs are clear. Vessels in both hila noted to be prominent. Upper lobe redistribution of pulmonary flow can be seen.
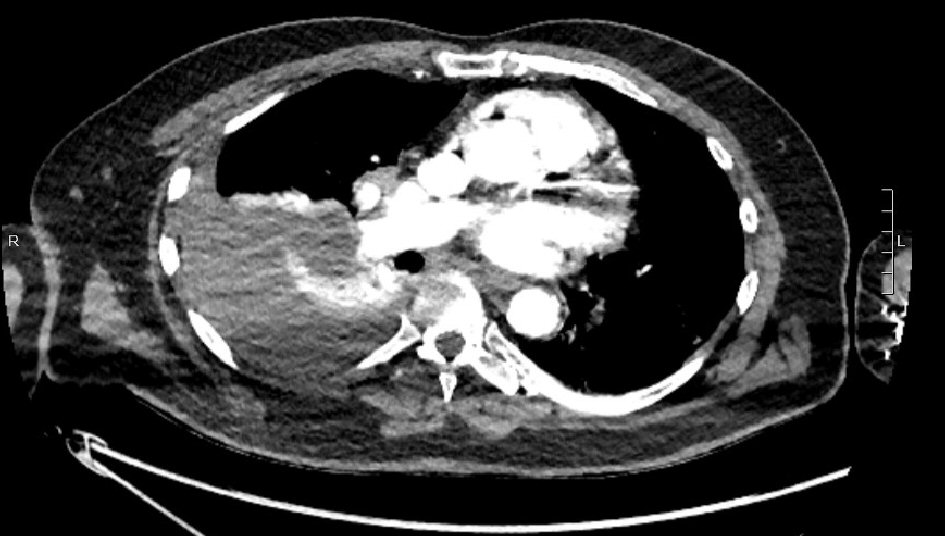
Figure 3. Thin slice from CT pulmonary angiogram showing large right-sided pleural collection (clinically hemothorax).
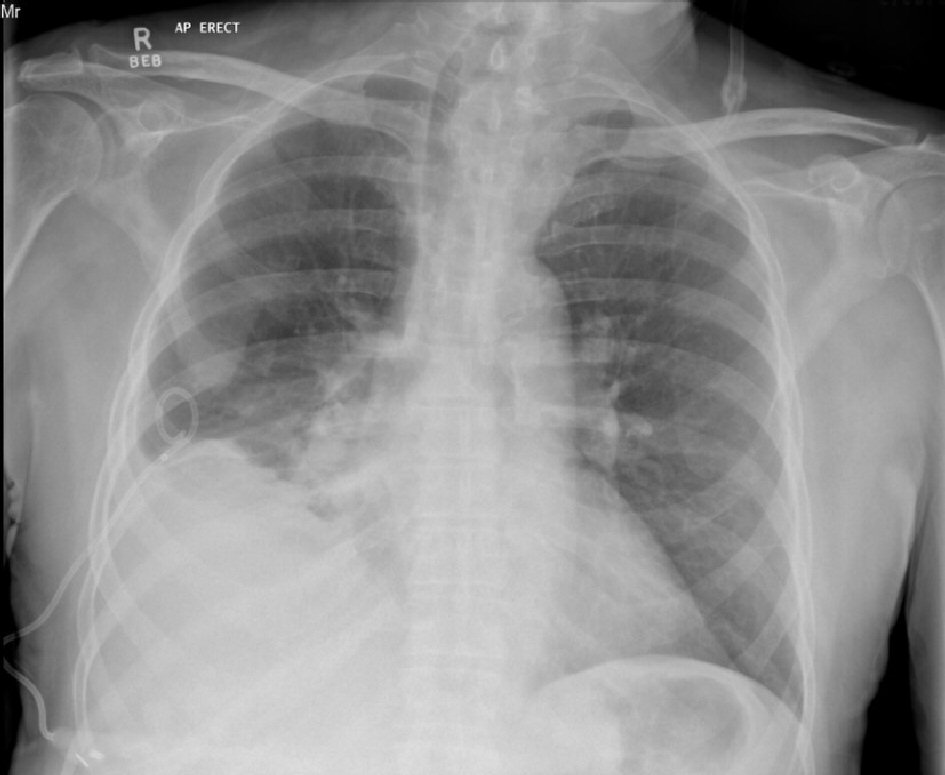
Figure 4. AP erect chest X-ray 7 days after intercostal catheter insertion for right pleural effusion. No ongoing drainage. Evidence of clearing of parenchymal changes compared to initial X-rays (Fig. 1).
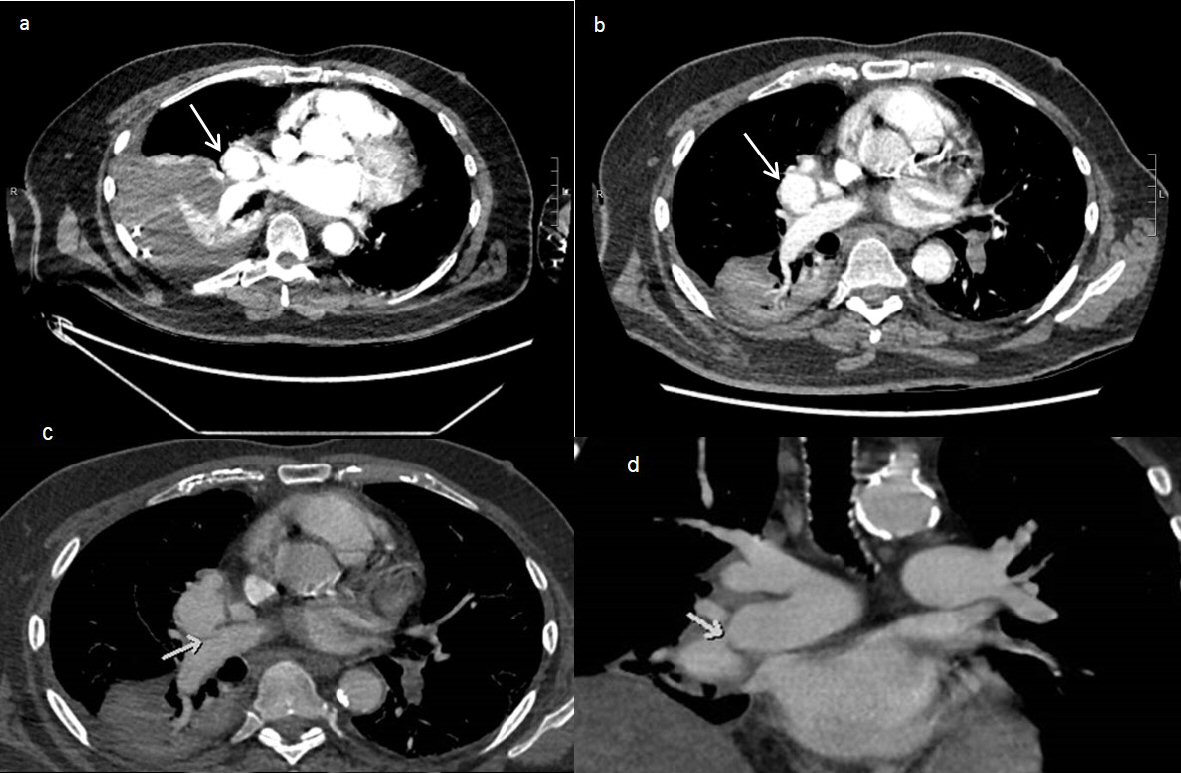
Figure 5. (a) CT pulmonary angiogram on day 6 of patient presentation showing a pulmonary artery pseudoaneurysm (arrow) measuring 35 × 32 × 35mm (AP × Transverse × CC). Note presence of large right-sided pleural collection with adjacent atelectasis. (b) CT pulmonary angiogram on day 12 of patient presentation showing growth of the pseudoaneurysm (arrow), measuring 39 × 35 × 40mm. There is a decrease in the size of the right pleural collection, showing a slightly loculated appearance. (c) Axial post contrast CT showed a large pseudoaneurysm arising from the distal right main pulmonary artery with homogenous contrast filling. The arrow showed the small connection between the pseudoaneurysm and the right pulmonary artery. (d) Coronal post contrast CT demonstrating the large pseudoaneurysm arising from the distal right main pulmonary artery (arrow), abutting the left atrium and right hemidiaphragm.
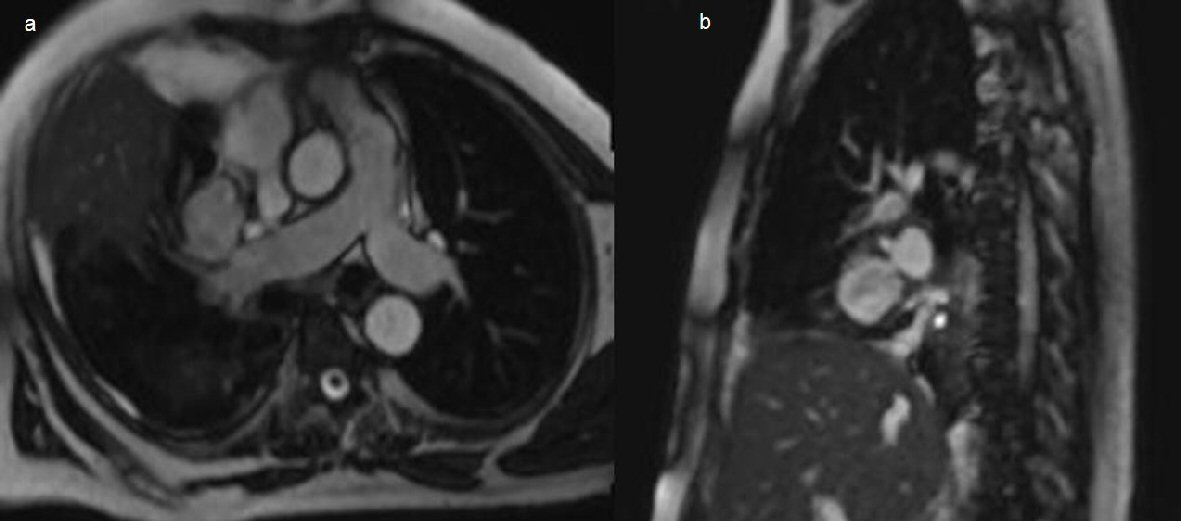
Figure 6. (a) Chest axial oblique non contrast MRI steady state free precession sequences showing a right pulmonary artery pseudoaneurysm arising from the medial segmental branch of the middle lobe, measuring 37 × 32 × 37mm. (b) Sagittal imaging through the pseudoaneurysm confirming connection to the right pulmonary artery.

Figure 7. Digital subtraction angiography. (a) Pre-embolization angiogram demonstrating contiguous flow between the pseudoaneurysm and the middle lobe artery. (b) The microcatheter and contrast within the lumen of the pseudoaneurysm. (c) Final post coiling imaging revealing complete occlusion of the pseudoaneurysm after successful embolization with Concerto coils without discernible residual contrast filling.