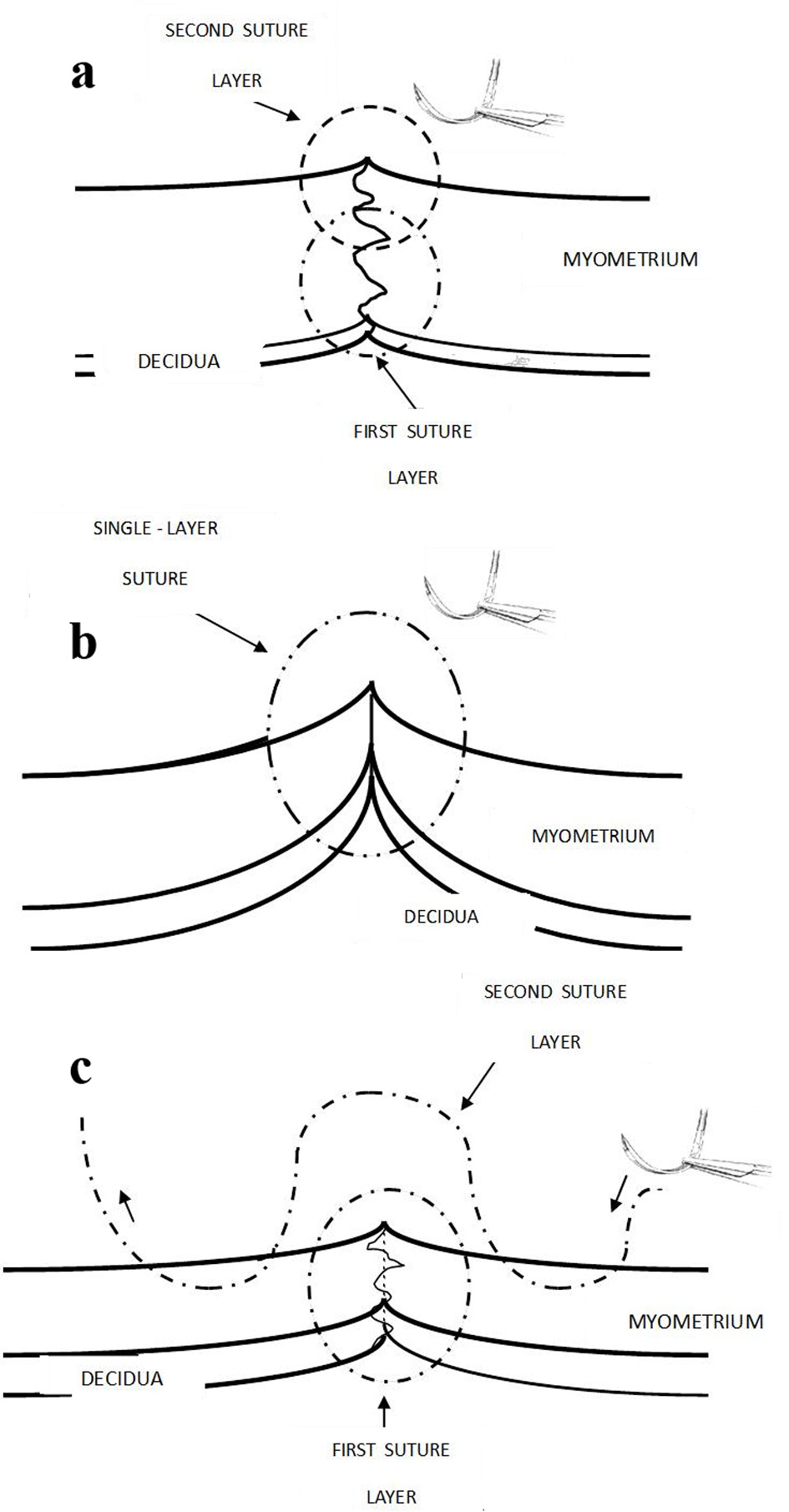
Figure 1. (a) Recommended traditional judicious double layer closure with the first continuous non-locking suture to include minimal decidua (< 5 mm) and about two-thirds of inner myometrium; and second non-locking suture taking upper half of myometrium would correct eversion of myometrial edges. This used to be the long-standing practice in UK more than a decade ago. Care should be taken not to make the edges of the incision ischemic. (b) One-layer closure could interpose decidua in between inner myometrium and the superficial myometrial edges can often be seen to be everted (not in good apposition). (c) The current popular technique in UK. The transverse myometrial bites of second layer are taken with the needle travelling back and forth on either side of incision which seem partly akin to “figure-of-eight” haemostatic/devascularizing sutures. It is easy to be paradoxically reassured by the apparent (excessive) apposition and sense of security derived from very tight sutures. Ischemic necrosis is likely to be causative in CS defect.