
Figure 1. Non-contrast abdominal CT demonstrating widespread colonic distension and air-fluid levels along with numerous areas of submucosal gas in the colonic wall.
| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 9, Number 7, July 2017, pages 654-658
Gastrointestinal Tract Amyloidosis Presenting With Pneumatosis Intestinalis
Figures
Table
| Yanamoto et al [8] | Khalid et al [5] | Pearson et al [7] | Current study | |
|---|---|---|---|---|
| Age, gender | 63-year-old male | 46-year-old male | 76-year-old male | 86-year-old male |
| Clinical presentation | Nausea, vomiting, diarrhea, and 10-year history of rheumatoid arthritis | Diffuse abdominal pain, melena, weight loss, dyspepsia | Postprandial bloating, periumbilical abdominal pain, weight loss | Abdominal pain, distention, and constipation |
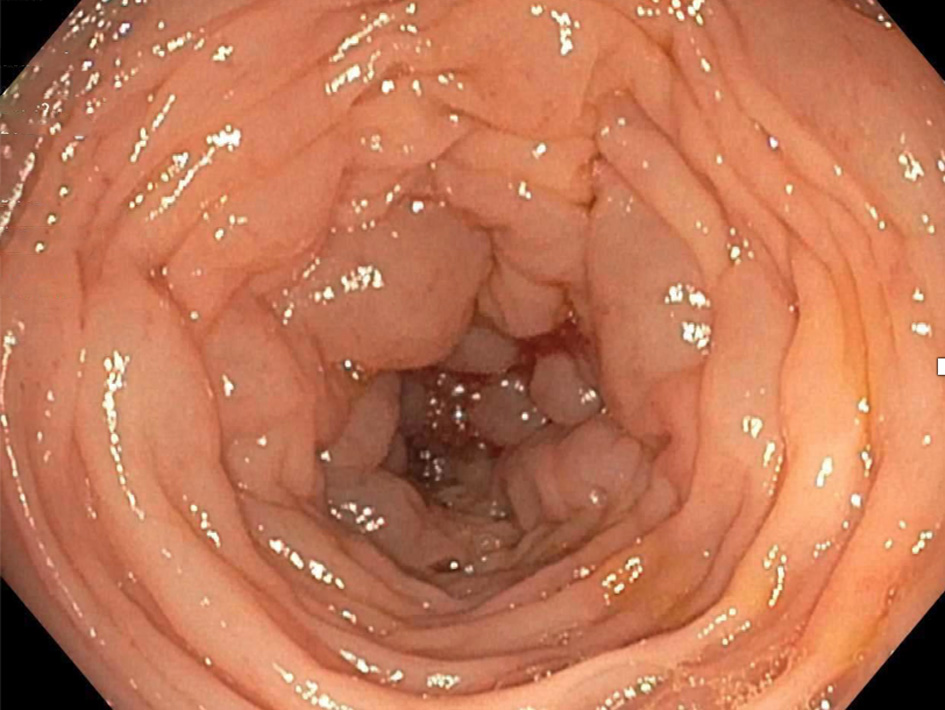
| Radiographic studies | CT abdomen/pelvis: gas pockets in portal venous system, pancreas, gut wall, and free peritoneal air | KUB: air fluid levels, free air under right hemidiaphragm. CT abdomen/pelvis: extensive pneumoperitoneum with focal dilation of small bowel loop. | KUB: pneumoperitoneum and pneumatosis intestinalis of small bowel. CT abdomen: pneumoperitoneum, pneumatosis intestinalis of small bowel, and gas in portal venous system. | CT scan showed diffuse colonic distension with submucosal gas pockets and numerous polypoid mucosal lesions with bowel wall thickening but no portal venous air or free intra-abdominal air. There was no whirl sign. |
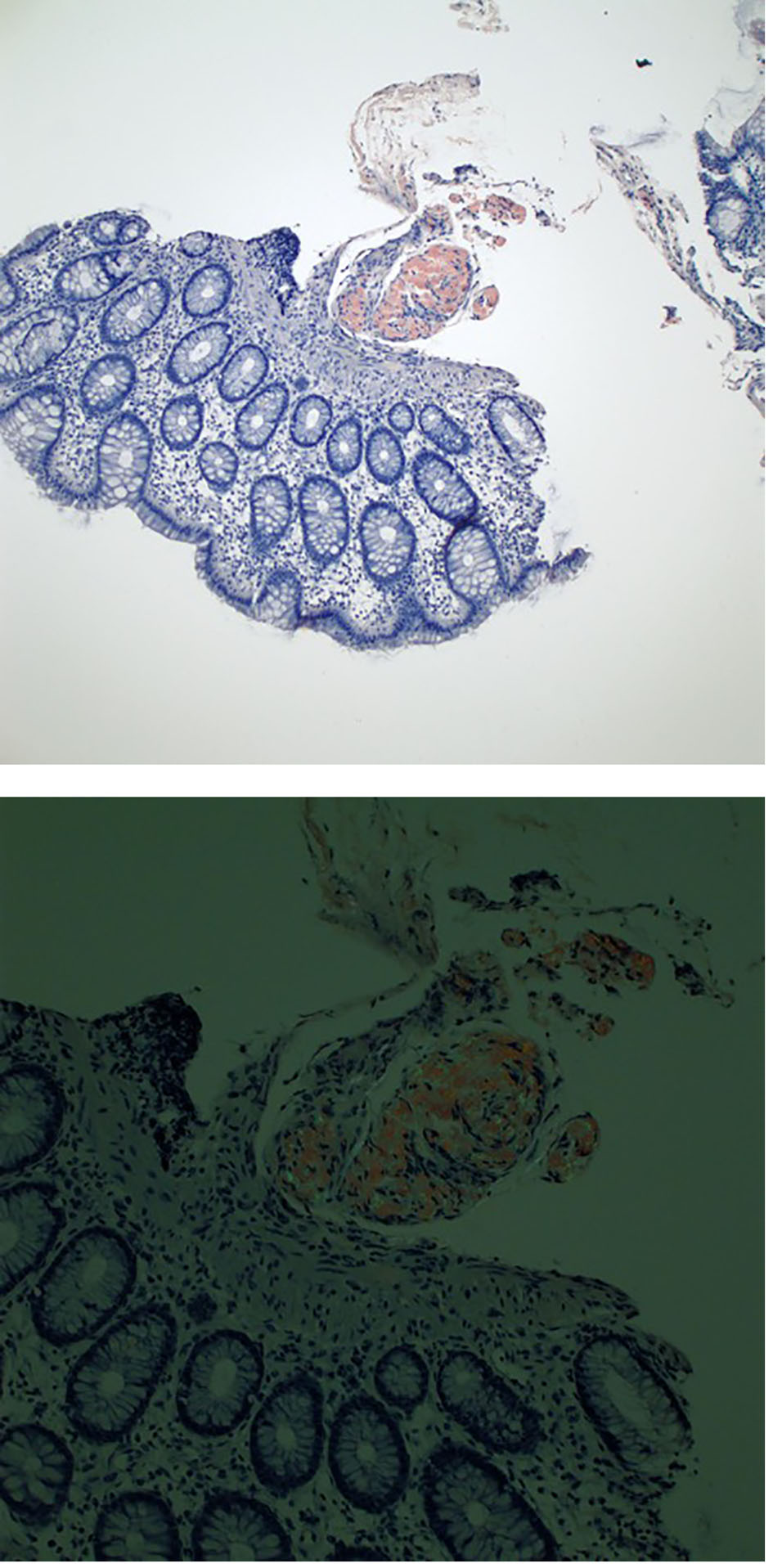
| Diagnosis | Secondary AA amyloidosis of GIT associated with rheumatoid arthritis. Hepatic portal vein gas and pneumatosis intestinalis. | Amyloidosis of GIT, sub-type unknown | IgG kappa multiple myeloma. Amyloidosis of GIT sub-type unknown. | Lambda light chain multiple myeloma. AA amyloidosis and ATTR amyloidosis of GIT. |
| Outcome | Pneumatosis intestinalis resolved with conservative management. Long-term outcome unknown. | Exploratory laparotomy showed no bowel perforation. Patient recovered with conservative management. Long-term outcome unknown. | Exploratory laparotomy with 4 cm small bowel resection. Died 15 months after surgery from recurrent small bowel obstruction. | Symptoms resolved with conservative management |