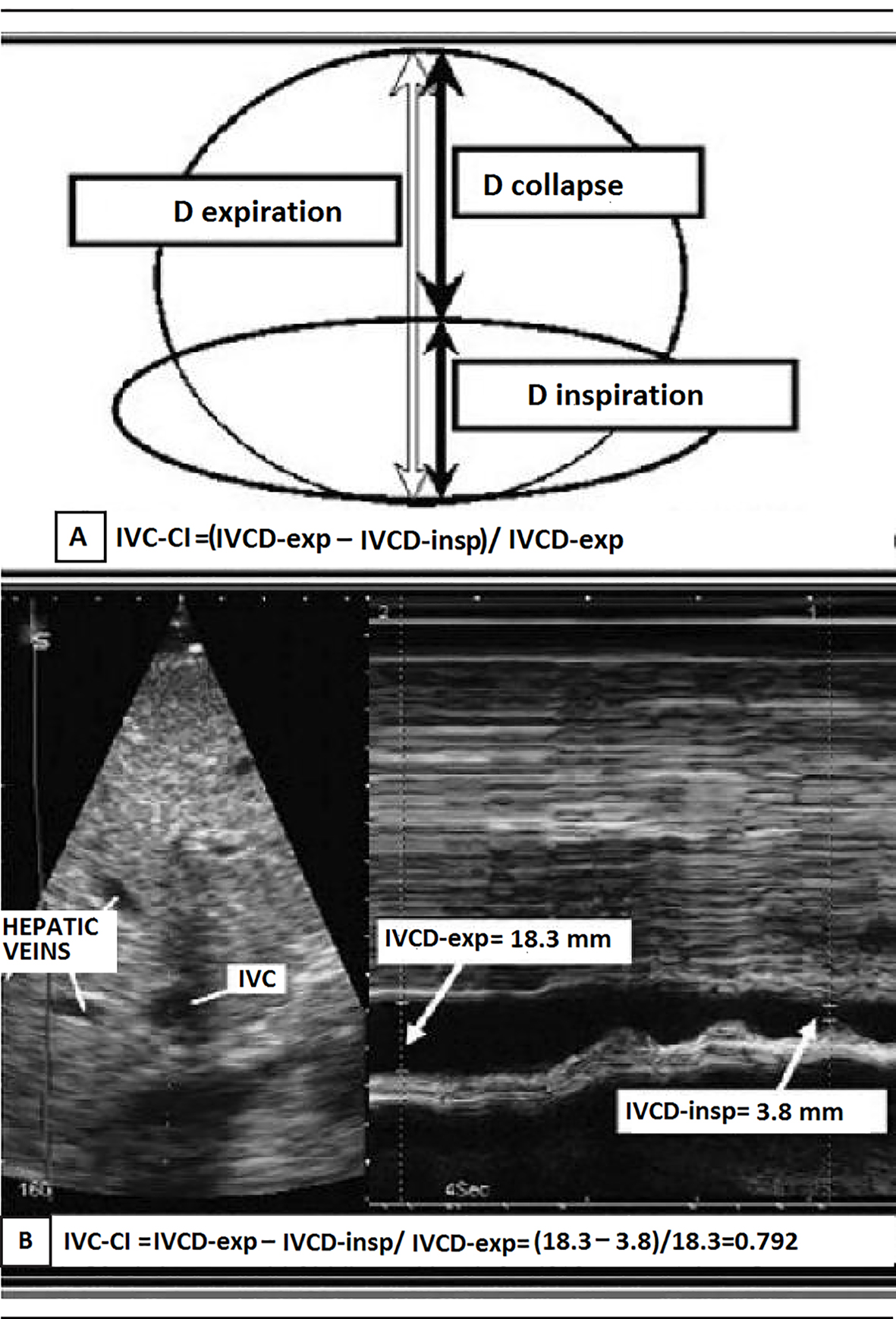
Figure 1. (A) Representation of the IVC collapsibility index (IVCCI) and (B) IVCCI measurement using M-mode ultrasonography. (A) IVCCI consists of the difference between the end-expiratory (IVCd-exp) and end-inspiratory (IVCd-insp) divided by IVCd-exp. (B) Based on the measurements in this example, the IVCCI would be (18.3 - 3.8 mm)/18.3 mm, or 79.2%.
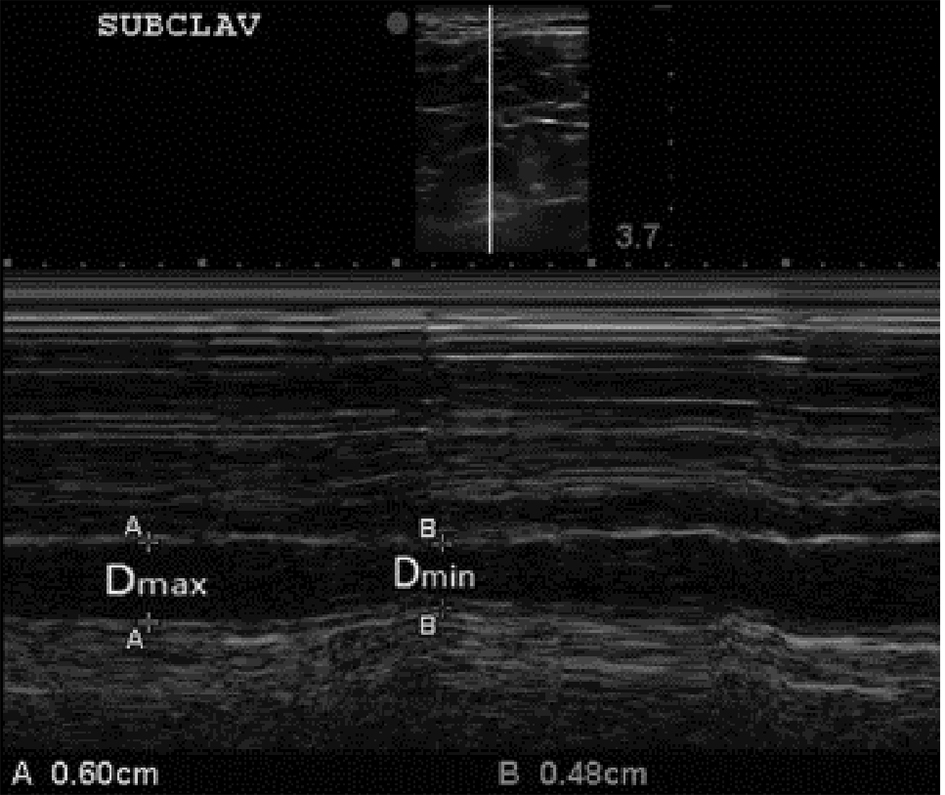
Figure 2. B-mode and M-mode views of the subclavian vein (SCV) with expiratory and inspiratory diameters measured. The clavicle is visualized anterior (above) the subclavian artery at the left side of the top image (superior to the SVC). Again, consistent with our approach to the IVCCI, we utilized minimal (inspiratory) and maximal (expiratory) diameters of the SCV. For further explanations, please see the text.