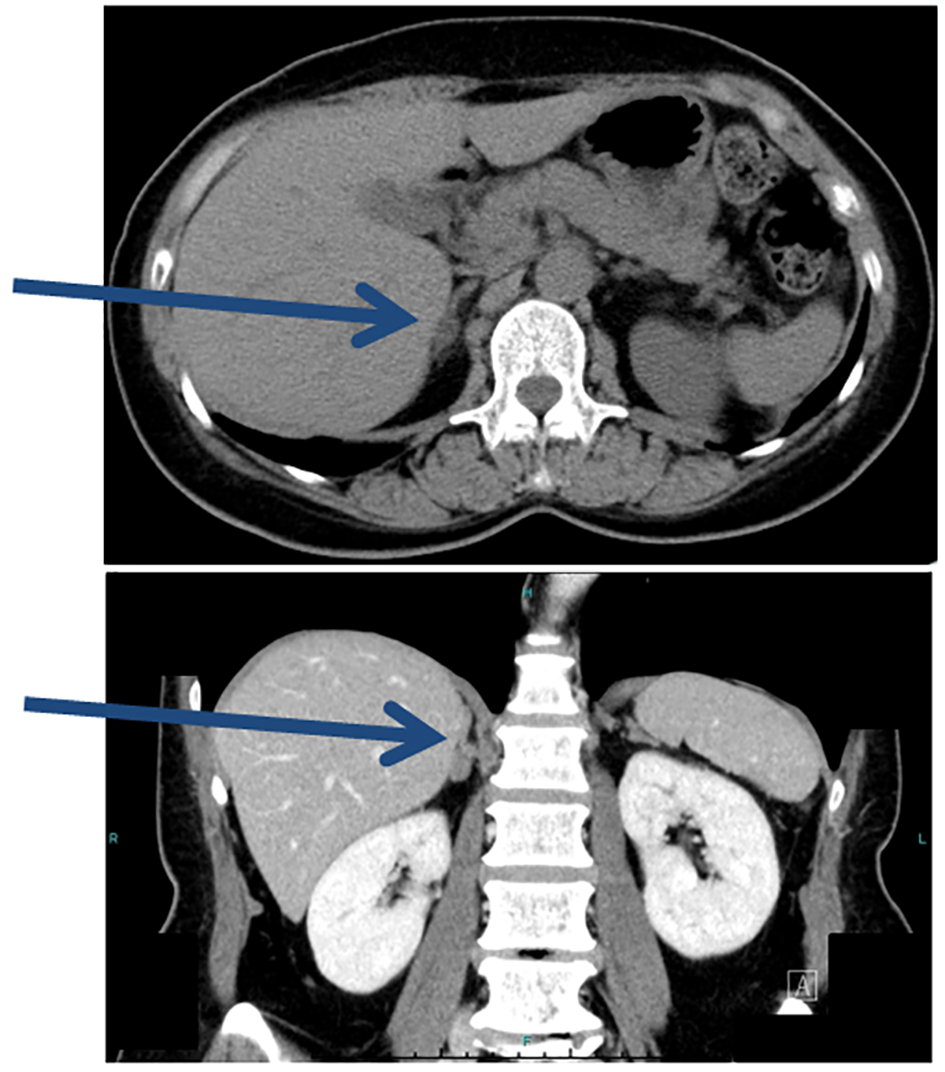
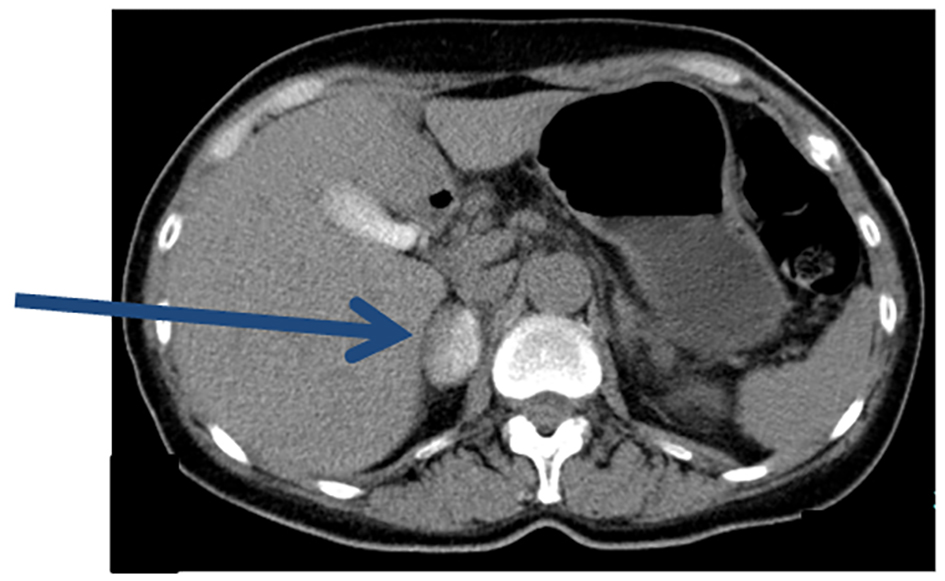
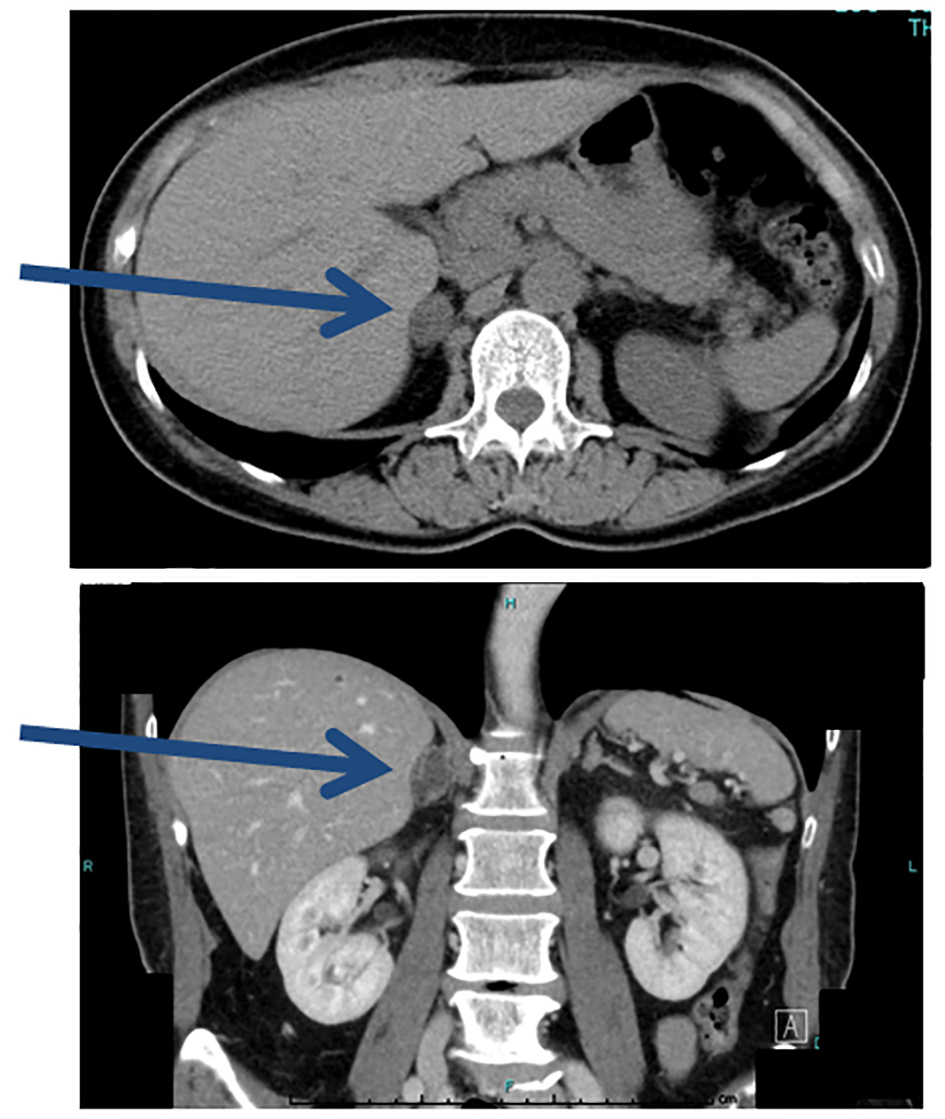
Figure 1. Plain CT prior to AVS. CT detected an adrenal mass 1.4 cm in diameter (arrows).
| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Case Report
Volume 10, Number 1, January 2018, pages 66-71
Persistent Primary Aldosteronism Despite Iatrogenic Adrenal Hemorrhage After Adrenal Vein Sampling
Figures
Table
| Before AVS (nifedipine 40 mg) | 2 weeks after AVS (nifedipine 40 mg) | After adrenalectomy (no medication) | |
|---|---|---|---|
| PR: pulse rate; PRA: plasma renin activity; PAC: plasma aldosterone concentration; ARR: aldosterone-renin ratio. | |||
| SBP, mm Hg | 136 | 137 | 121 |
| DBP, mm Hg | 80 | 95 | 83 |
| PR, bpm | 78 | 92 | 67 |
| PRA, ng/mL/h | 0.2 | 0.1 | 0.4 |
| Cortisol, µg/dL | 9.9 | 9.1 | 7.2 |
| PAC, pg/mL | 355 | 105 | 124 |
| ARR | 1,775 | 1,050 | 310 |