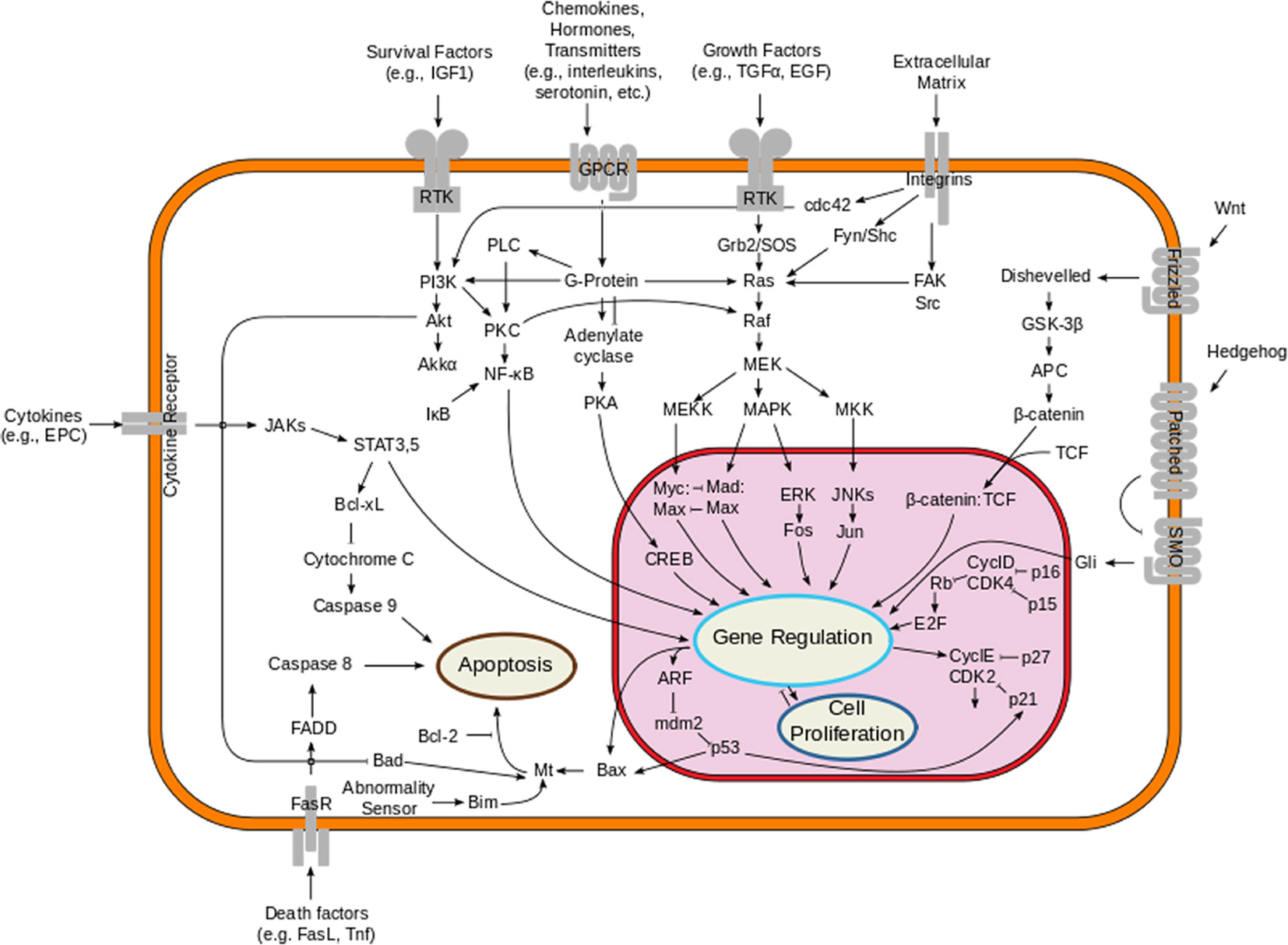
Figure 1. Overview of the signal transduction pathway like mitogen-activated protein kinase/extracellular signal-regulated kinases signaling pathway.
| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Review
Volume 8, Number 2, February 2016, pages 63-75
Novel Drugs and Combination Therapies for the Treatment of Metastatic Melanoma
Figure
Table
| Treatment related adverse effects | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|---|---|---|---|
| AST: aspartate aminotransferase; ALT: alanine aminotransferase; ULT: upper limit of normal. | ||||
| Skin toxicity. Most common adverse effect. | Mild to moderate localized rash or pruritus; papules/pustules covering < 10-30% of body surface. Rx: topical corticosteroids. | Non-localized rash (diffuse, ≤ 50% of skin surface) Rx: topical corticosteroids and monitoring. | Intense or widespread rash > 30%; skin sloughing < 10-30% of body surface; epidermal or mucus membrane detachment. Rx: systemic corticosteroids, hospitalization and hold immunotherapy. | Stevens-Johnson syndrome, toxic epidermal necrolysis (1% of cases), or rash complicated by full-thickness dermal ulceration, bullous and blisters. Rx: immediate hospitalization, systemic steroids and discontinue drug permanently. |
| GI toxicity/diarrhea. Second most common | < 4 stools per day over baseline Rx: symptomatic treatment. | 4 - 6 stools per day over baseline. Rx: IV fluids for < 24 h, and symptomatic treatment. Rule out infectious causes. If not improving, hold drug and consider oral/IV steroids. | ≥ 7 stools per day over baseline. Rx: IV fluids for > 24 h, hospitalization and IV steroids. | Life-threatening consequences (e.g., hemodynamic collapse). Rx: hospitalization, IV fluids, IV steroids. If symptoms not improving with IV steroids, consider infliximab. |
| Hepatotoxicity. Occurs in about 10% of patients. | Asymptomatic or mild symptoms. Rx: clinical or diagnostic observations only; intervention not indicated | AST or ALT > 2.5 to ≤ 5.0× ULN and/or total bilirubin > 1.5 to ≤ 3.0× ULN. Rx: frequent monitoring of LFTs. Consider holding immunotherapy. | AST or ALT > 5× ULN and/or total bilirubin > 3.0× ULN. Rx: hold immunotherapy and frequent monitoring of LFTs. Rule out viral, autoimmune or drug induced hepatitis. | High ammonia levels and hepatic encephalopathy. Rx: discontinue drug permanently and start high dose steroids (2 mg/kg/day). If not improving in 48 h, consider oral mycophenolate (500 mg twice daily). |
| Endocrine toxicity. Occurs in 4-8% of patients. | Asymptomatic. Rx: clinical or diagnostic observations only; intervention not indicated | Moderate symptoms. Rx: if suspicious for hypophysitis is high, complete endocrine workup should be done. Hormone replacements may be considered. | Severe symptoms. Rx: hospitalization indicated. Stop immunotherapy. Short course of steroids may improve pituitary function. | Adrenal crisis: severe dehydration, hypotension, or shock. Life-threatening consequences Rx: high dose IV steroids. |