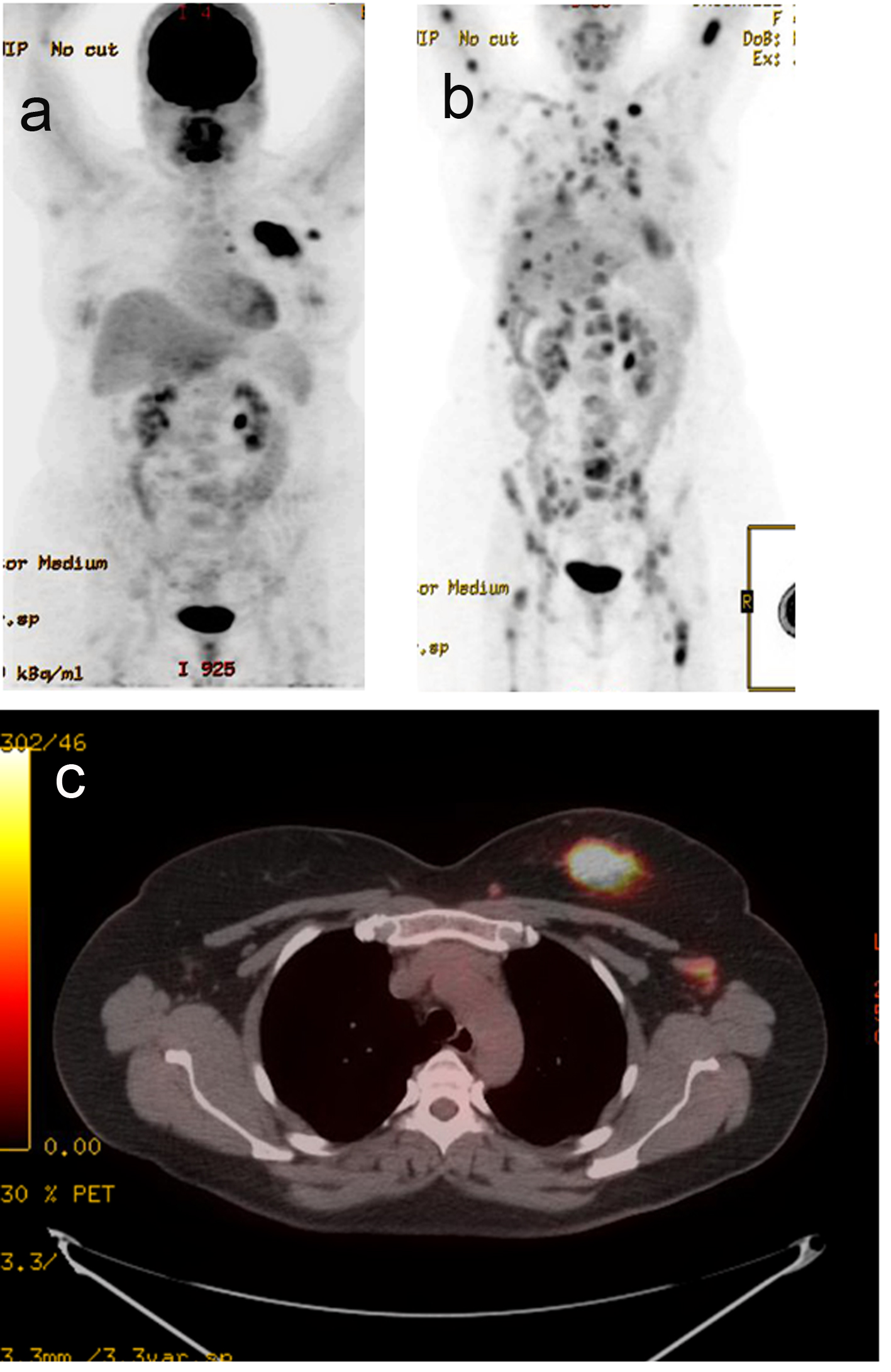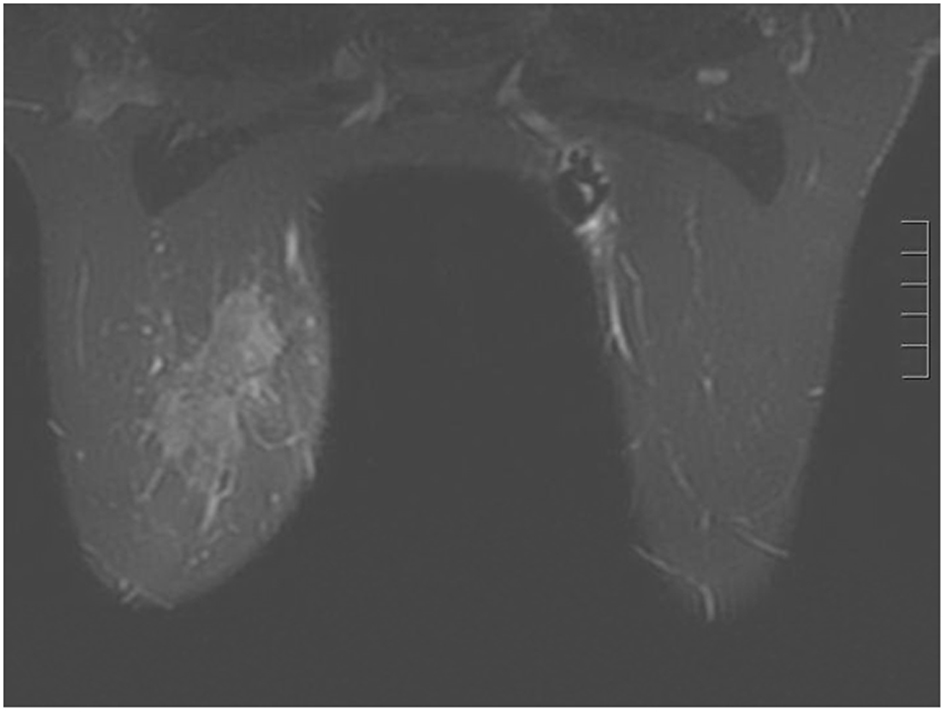
Figure 2. Breast MRI 2012. Given the large triple negative cancer, a breast MRI and PET-CT scan were performed for staging purposes. The PET-CT showed a 5 cm left breast mass which was FDG-avid, as well as an 8 mm left axillary LN and a 5 - 6 mm left internal mammary node both also FDG-avid. No distant metastasis was evident. The left axillary LN underwent an ultrasound-guided biopsy that proved metastatic from the breast. The breast MRI showed a 7.1 × 3.3 cm enhancing mass at the left breast 10:00 - 11:00 position, and a 2.8 cm axillary LN, both of which are already biopsy-proven malignancies. After workup, the patient’s final clinical stage was cT3 N3 M0 - stage IIIC. A multidisciplinary breast conference was held and the group decided that treatment should include neoadjuvant chemotherapy, surgery, whole breast RT including regional basins, and genetic counseling for BRCA testing. The patient underwent six cycles of TAC (docetaxel, doxorubicin and cyclophosphamide) which she finished in January 2013. BRCA testing revealed no mutation in the BRCA 1 and 2 genes. The post-chemotherapy physical exam showed excellent clinical response with no palpable evidence of disease in the left breast. Breast MRI and PET-CT (February 2013) both also showed complete clinical response (both breast tumor and lymphadenopathy). Brain MRI also showed negative findings.