Figures

Figure 1. Photo showed deceleration of growth (-3 SD) and peculiar craniofacial and oral abnormalities such as sparse skull hair, frontal bossing, depressed nasal bridge and hypertelorism and epicanthic folds. Patient manifested bifid nose with hypoplasia of the alae and a short philtrum and a median partial cleft lip and an operated unilateral paramedian cleft and lobated tongue with a papilliform protuberance and hamartoma of the ventral surface of the tongue.
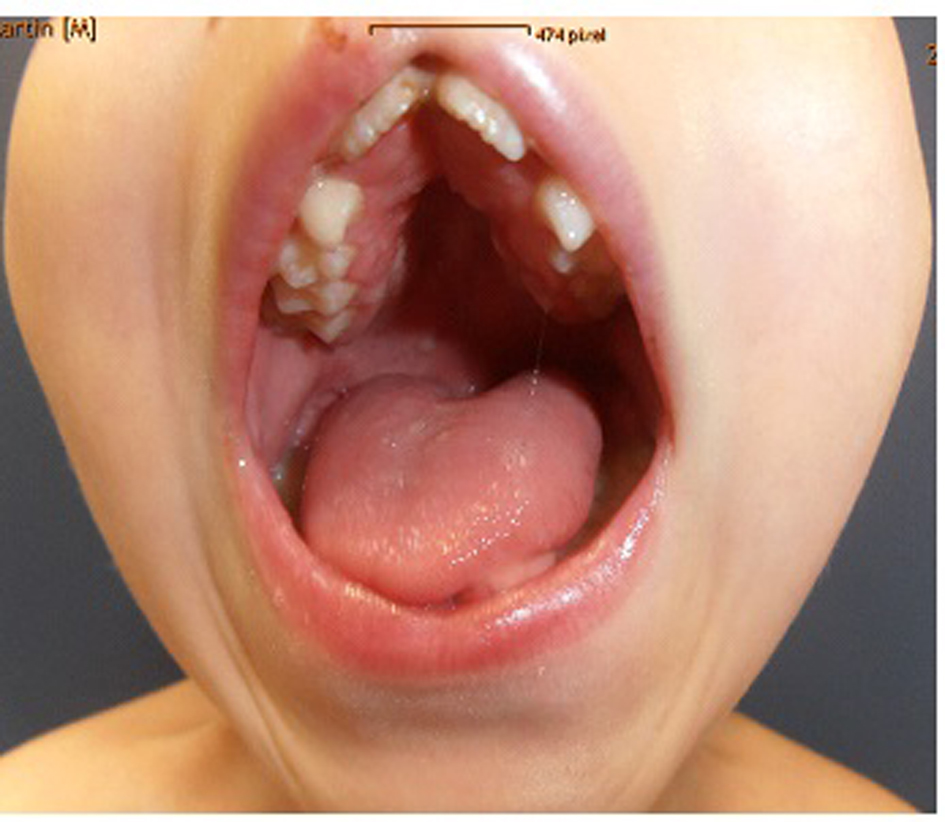
Figure 2. Flattening of the alveolar crest with a median sulcus and several nodules and a cleft palate associated with gingival fibromatosis, fusion of the lateral incisors (bilaterally). Ears were large, low-set and showed ill-defined modeling.

Figure 3. The hands were short with clinodactyly of the fifth fingers and his bilateral postaxial hexadactyly were operated early on. The feet were short with duplication of the hallux (polysyndactyly). Anteroposterior radiograph of the hands showed bilateral ulnar deviation, unilateral synostosis of the right third and fourth metacarpals, and marked dysplasia of the intermediate phalanges bilaterally.

Figure 4. Lateral skull radiograph showed obtuse angle of the mandible, wormian bones, hypoplasia of the zygoma, mandible and maxilla respectively.

Figure 5. Lower limb standing radiograph showed a hypoplastic iliac bones, severe coxa valga, associated moderate subluxation of the hip because of incomplete development of the acetabulae with over-tubulation of the long bones.