Figures

Figure 1. Pre-operative view demonstrating limited mouth opening and swelling in the right temporomandibular joint area.

Figure 2. Coronal CT (bone window) depicts expansion of the right mandibular condyle by a soft tissue cancellous lesion with partial interruption of cortical bone and marked shortening of ascending ramus. Note lack of intraosseous trabeculae or calcification.
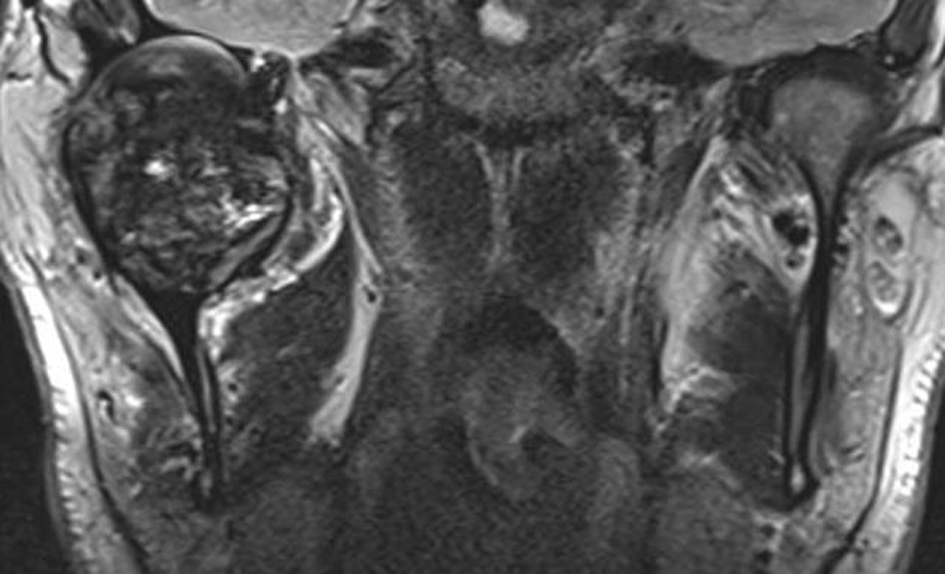
Figure 3. Coronal MR (T2w) delineates an intraosseous soft tissue tumor with considerable intratumoral low signal (black color) indicating hemosiderin components. Articular surface of glenoid fossa is preserved. The joint capsule is markedly expanded.
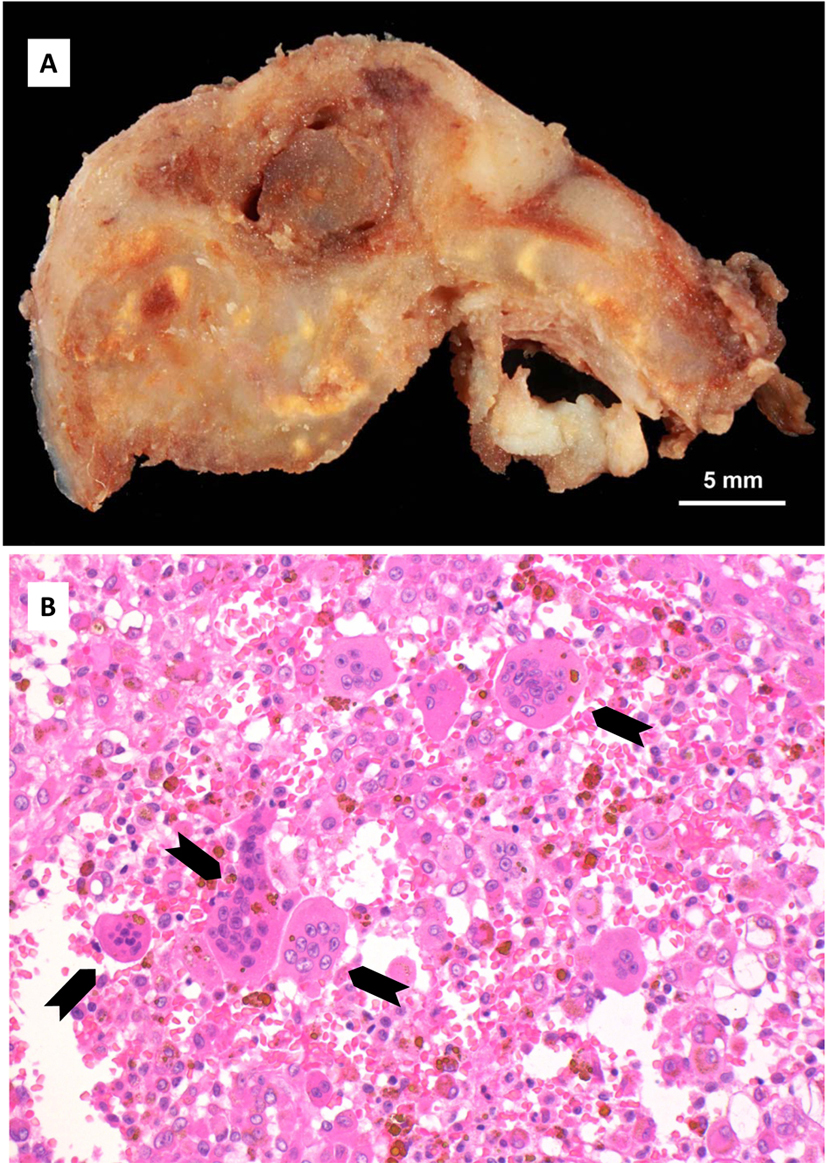
Figure 4. Histopathology: (A) Cut surface of the tumor, demonstrating locally destructive lesion with heterogeneous gross pattern. (B) Microscopically, giant cells (arrows) containing proliferation of mononuclear cells with abundant brown hemosiderin pigment (hematoxylin and eosin stain, original magnification × 200).
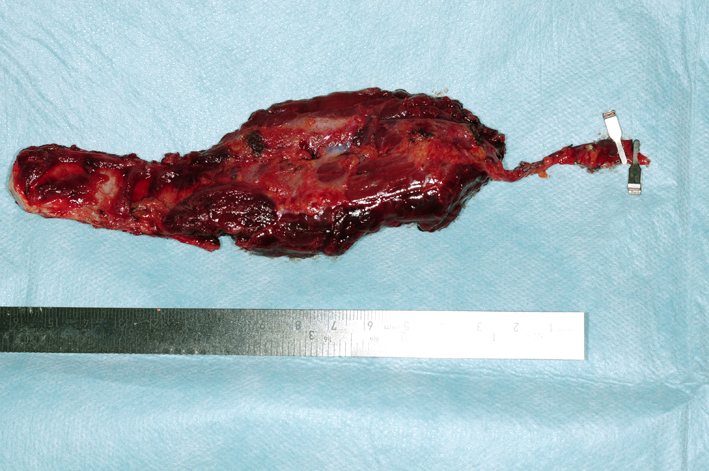
Figure 5. Vascularized costochondral graft and part serratus anterior muscle based on the thoraco-dorsal artery.
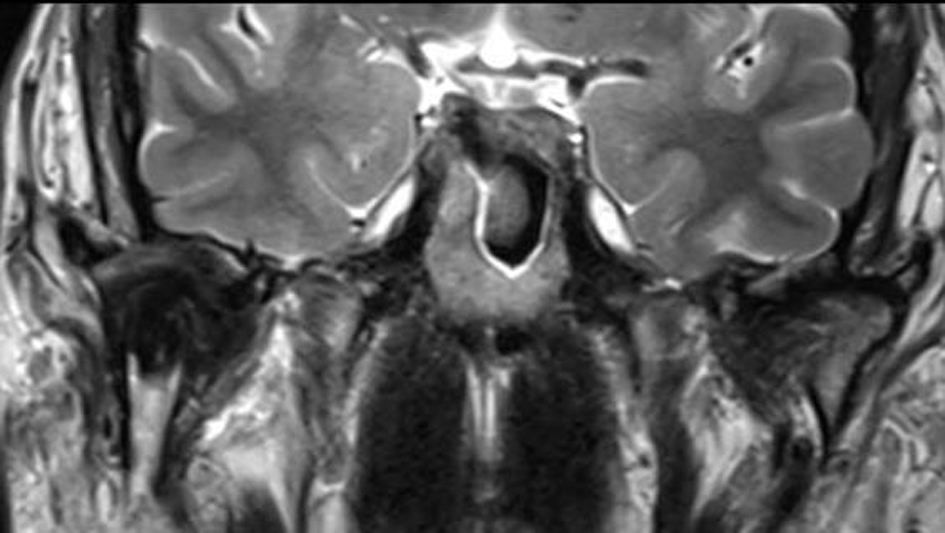
Figure 6. Post-operative MR (T2w) 1 year following shows the costochondral bone graft that due to remodeling abuts a well maintained joint space without evidence of recurrence.

Figure 7. Post-operative view demonstrating improved mouth opening and condylar movement.