











| Journal of Clinical Medicine Research, ISSN 1918-3003 print, 1918-3011 online, Open Access |
| Article copyright, the authors; Journal compilation copyright, J Clin Med Res and Elmer Press Inc |
| Journal website http://www.jocmr.org |
Original Article
Volume 10, Number 3, March 2018, pages 226-232
Stress Factors Associated With Burnout Among Attending Physicians: A Cross-Sectional Study
Yurika Kawamuraa, e, Ayumi Takayashikia, b, Makoto Itoc, Takami Maenoa, b, Emiko Seoa, b, d, Tetsuhiro Maenoa, b, d
aGraduate School of Comprehensive Human Science, University of Tsukuba, Tsukuba, Ibaraki, Japan
bDepartment of Primary Care and Medical Education, Faculty of Medicine, University of Tsukuba, Tsukuba, Ibaraki, Japan
cNational Hospital Organization, Kasumigaura Medical Center, Tsuchiura, Ibaraki, Japan
dCenter of Medical Education and Training, University of Tsukuba Hospital, Tsukuba, Ibaraki, Japan
eCorresponding Author: Yurika Kawamura, University of Tsukuba, 1-1-1 Tennodai Tsukuba Ibaraki 305-8575, Japan
Manuscript submitted December 6, 2017, accepted December 22, 2017
Short title: Stress Factors Associated With Burnout
doi: https://doi.org/10.14740/jocmr3299w
| Abstract | ▴Top |
Background: Burnout in attending physicians is a crucial issue that may negatively impact patient outcomes, as well as affect the quality of training provided to residents. To investigate the association between burnout and stress-coping ability, we conducted a cross-sectional study of attending physicians.
Methods: From April 2013 to March 2014, we distributed an anonymous, self-administered questionnaire to 1,897 attending physicians who attended teaching-related training sessions and workshops. The questionnaire included the Maslach Burnout Inventory General Survey (MBI-GS, Japanese version) to evaluate burnout; the sense of coherence scale (SOC, Japanese version) to measure stress-coping ability, with higher scores indicating higher stress-coping ability; the Brief Scales for Job Stress (BSJS) to assess stress and buffering factors; demographic factors; mean weekly working hours; and factors related to instructing residents. The MBI-GS was used to determine the presence of physician burnout. Subjects were divided into tertiles based on SOC scores. We conducted logistic regression analysis of burnout using the following independent variables: physician experience, sex, mean weekly working hours, SOC group, mental workload, and reward from work.
Results: Of the 1,543 (81.3%) attending physicians who responded, 376 did not meet the inclusion criteria and 106 had missing data, thus 1,061 (55.9%) were analyzed. The prevalence of burnout was 17.2%. Physicians with burnout had significantly fewer years of experience as a doctor (P < 0.01), were more likely to be female (P < 0.01), worked more hours per week (P < 0.01), and had a lower SOC score (P < 0.01) than physicians without burnout. On the BSJS, the mean score of all stress factors was higher and that of buffering factors was lower in physicians with burnout (P < 0.01). The percentages of physicians with burnout were 35.7%, 12.8%, and 3.2% in the low, middle, and high SOC groups, respectively (P < 0.01). Using the high SOC group as a reference, the adjusted odds ratio for burnout in the low SOC group was 4.7 (95% confidence interval: 2.31 - 9.63) (P < 0.01).
Conclusions: In this study, burnout among attending physicians was significantly associated with SOC scores after adjustment for stress factors and buffering factors.
Keywords: Burnout; Attending physician; Sense of coherence; Individual factors; Stress factors; Buffering factors; Work hours; Mental health
| Introduction | ▴Top |
Burnout, a mental reaction to stress at the workplace, is a critical concern. Emotional exhaustion due to increasing stress can reduce individuals’ interest in or passion for their work, negatively impact performance, and ultimately lead to depression.
A previous study showed that physician burnout can have a negative influence on clinical performance [1]. Attending physicians play two simultaneous roles, namely taking care of patients and instructing medical residents. Therefore, the negative influence of burnout on the performance of attending physicians may worsen patient outcomes and affect the quality of training provided to residents.
Previous studies reported that 34% of faculty physicians [2] and 28.7% of internal medicine residency program directors experienced burnout [3]. In Japan, 36.1% of “interpersonal professionals” (including physicians, nurses, teachers, and social workers) [4] and 21.8% of physicians working in stroke care suffered from burnout [5], but there are no previous studies on burnout in attending physicians. Clarifying the rates of burnout and associated factors in this population will facilitate early detection and provision of more effective prevention strategies.
Burnout is a stress reaction included in one of the most widely used occupational stress models, developed by the National Health Institute for Occupational Safety and Health (NIOSH). This model suggests that stress factors, buffering factors, and individual factors exert a marked influence on stress reactions [6, 7]. Many previous studies were conducted on stress factors and buffering factors [5, 8-11]. Regarding stress factors, long working hours were significantly associated with burnout among surgeons [8] and psychiatric trainees [9]. Concerning buffering factors, Linzer et al demonstrated that low work control was one predictor of burnout among physicians [11].
Compared to the other two factors influencing stress reactions, individual factors have not been as well investigated. Sense of coherence (SOC), used as a measurable individual factor in many studies, is a concept proposed by Antonovsky in 1979. It consists of three components: the ability to clearly understand and accept one’s problems; the ability to cope with these problems successfully; and the ability to assign meaning to these problems, seeing them as worthy of commitment and engagement [12]. Antonovsky developed the SOC scoring system in 1987, and it has subsequently been used as a tool to measure the ability to cope with stress [12].
A previous study in Greece examined burnout and SOC, and found that nurses who had a high SOC score, which is an individual factor that reflects stress-coping ability, were less likely to experience burnout [13]. However, that study did not consider stress factors or buffering factors, so it is unclear whether adjustment for these factors would eliminate the association between individual factors and burnout. Another study of Japanese medical residents suggested that there was an association between SOC and depression even after adjusting for stress factors and buffering factors [14]. However, since the outcome was depression rather than burnout, and the subjects were residents who were still in training, it is unknown whether these findings are generalizable to attending physicians.
We therefore a conducted a cross-sectional study to investigate the association between burnout and SOC in attending physicians after adjusting for both stress factors and buffering factors.
| Materials and Methods | ▴Top |
Subjects and study design
We recruited attending physicians who played a role in instructing first- and second-year residents. In Japan, this role requires attendance at training sessions and workshops that take place nationwide. From April 2013 to March 2014, we asked all 135 organizers of these events to participate in the present study; of these, 75 (55.5%) replied and 48 (35.6%) participated. The organizers distributed the self-administered study questionnaire to 1,897 attending physicians who attended the training sessions and workshops. All participants remained anonymous.
Questionnaire
The questionnaire consisted of the Japanese version of the Maslach Burnout Inventory General Survey (MBI-GS) to evaluate burnout; the Japanese version of the SOC scale to measure stress-coping ability; the Brief Scales for Job Stress (BSJS) to assess stress factors and buffering factors; demographic factors; mean weekly working hours; and factors regarding instructing residents.
MBI-GS
This is a 16-item questionnaire with three subscales, each of which uses a seven-point (0 - 6) rating scale, and is evaluated by the average score per subscale. The subscales measure exhaustion, cynicism, and professional efficacy [15]. In a previous study, an exhaustion score ≥ 4.0 and a cynicism score ≥ 2.6, or an exhaustion score ≥ 4.0 and a professional efficacy score ≤ 1.5, were used to define burnout [4]. Construct validity and reliability have been ascertained for the Japanese version of the MBI-GS [16].
SOC scale
The 13-item version of the SOC questionnaire uses a five-point rating scale, with a final score ranging from 13 to 65 [17]. Higher scores indicate better stress-coping ability. Because the SOC score does not have a definitive cut-off point, we divided subjects according to SOC score tertiles into low, medium, and high SOC groups [18]. The Japanese version of the 5-point SOC-13 has been tested previously for reliability and validity [17].
BSJS
The BSJS comprise six subscales: workload, mental workload, problems in personal relationships, job control, reward from work, and support from colleagues and superiors. The first three factors are perceived stress factors, whereas the rest are buffering factors. All items are rated on a four-point scale ranging from 1 to 4, and a mean score is calculated for each subscale [19]. For stress factors, high scores indicate high levels of stress, whereas high buffering factor scores mean a greater degree of stress buffering. These subscales have been demonstrated to have sufficiently high internal consistency [19].
Mean working hours
As in previous studies [14, 20, 21], we calculated mean weekly working hours using the following equation: 5 × (mean number of hours worked on weekdays) + 2 × (mean number of hours worked on weekends) + 7 × (number of night shifts per month/30) × (24 - mean working hours on weekdays).
Statistical analysis
In this study, we defined attending physicians as those with over 7 years of clinical experience, which is congruent with the official definition by the Japanese government, and those with opportunities to train residents. We excluded physicians who had less than 7 years of clinical experience and those who spent very little time instructing residents at the bedside. We also excluded physicians with missing data for any of the following: MBI-GS score, SOC score, BSJS score, and demographic information.
To reveal any associations between demographic information, mean working hours, SOC score, and BSJS score, we conducted Chi-squared tests (for categorical variables) or t-tests (for continuous variables) for each variable in the univariate analysis. We conducted binomial logistic analysis for burnout using demographic information and independent variables defined as those with P values of < 0.10 in the univariate analysis. To avoid collinearity in cases where a strong correlation exists between variables with significant effects, we sorted and selected one of those variables as the independent variable.
The significance level was set at P < 0.05. All statistical analyses were conducted using IBM SPSS Statistics for Windows version 22.0 (IBM Japan, Ltd, Tokyo, Japan).
Ethical considerations
This study was approved by the Ethics Committee of the Faculty of Medicine at the University of Tsukuba. All participants provided written informed consent. We also explained to all prospective respondents that their participation in the study was purely voluntary.
| Results | ▴Top |
Subject characteristics
We distributed the questionnaire to 1,897 attending physicians, 1,543 (81.3%) of whom responded. After excluding 28 subjects who did not have more than 7 years of experience and 352 who spent very little time instructing residents at the bedside (redundantly counted), as well as 58 subjects who did not provide information regarding experience or resident instruction, 1,109 remained. Forty-eight subjects with missing data were also excluded, resulting in a final analysis of 1,061 (55.9%) physicians. Of these, 892 (84.1%) were male. The mean age was 40.8 years, the mean duration of experience as a physician was 15.3 years, and the mean number of hours worked weekly was 79.3. The percentage of physicians working more than 80 h per week was 42.7%. Demographic information, mean weekly working hours, prevalence of burnout, SOC score, and BSJS score are shown in Table 1.
 Click to view | Table 1. Participant Characteristics, Mean SOC Scores, and Mean Working Hours (N = 1,061) |
SOC scores and grouping
The mean SOC score of the attending physicians was 44.5 (range: 16 - 65). In terms of categorization by SOC score, 359 (33.8%), 328 (30.9%), and 374 (35.2%) physicians were categorized in the low, medium, and high SOC groups, respectively.
Factors associated with burnout
Physicians with burnout, in comparison to those without, had fewer years of clinical experience (14.0 vs. 15.6 years; P < 0.01), were more likely to be female (22.5 vs. 14.6%; P < 0.01), and worked more hours per week (84.6 vs. 78.1 h/week; P < 0.01). The mean SOC score was significantly lower in physicians with burnout (37.8 vs. 45.8; P < 0.01). Finally, all stress factors were higher in physicians with burnout whereas all buffering factors were lower (P < 0.01) (Table 2).
Click to view | Table 2. Association Between Burnout and Demographic Information, Mean SOC Scores, Mean Working Hours, and BSJS Scores (N = 1,061) |
Relationship between burnout and SOC score
The percentages of physicians with burnout were 35.7%, 12.8%, and 3.2% in the low, middle, and high SOC groups, respectively (P < 0.01) (Fig. 1).
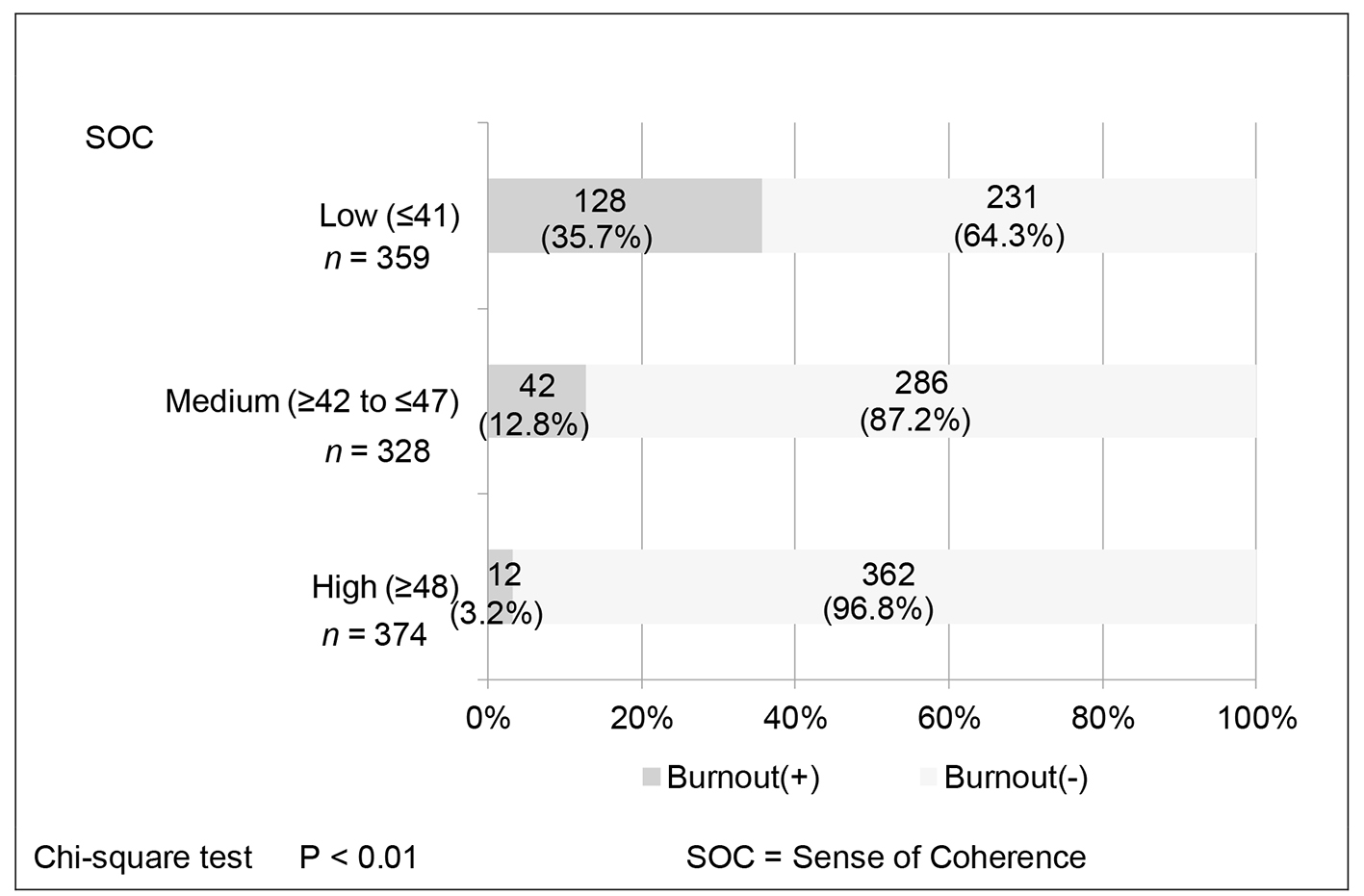 Click for large image | Figure 1. Relationship between burnout and the three SOC groups. |
Logistic regression analysis
The results of multivariate logistic regression analysis for burnout are shown in Table 3. Because all variables were significantly associated with burnout in univariate analysis, we calculated the correlation within variables and selected some variables to include as independent variables in the logistic analysis to avoid multicollinearity. Since there was a strong correlation between age and experience, we selected “experience as a physician” as the independent variable for the model. Correlations within the three stress factors (workload, mental workload, and problems in personal relationships) ranged from 0.220 to 0.643, and correlations within the three buffering factors (job control, reward from work, and support from colleagues and superiors) ranged from 0.360 to 0.529. Thus, to avoid collinearity, we selected “mental workload” as the independent variable representing stress factors, and “reward from work” to represent buffering factors. Consequently, we conducted logistic regression analysis using physician experience, sex, mean weekly working hours, SOC group, mental workload, and reward from work as independent variables. Using the high SOC group as the reference, the adjusted odds ratio (OR) (95% confidence interval (CI)) of the low SOC group for burnout was 4.7 (2.31 - 9.63), and that of the middle SOC group was 2.8 (1.32 - 5.76) (P < 0.01). When a reference value of < 60 h was used for mean weekly working hours, the adjusted OR for ≤ 100 h per week was 7.8 (2.20 - 27.4) (P < 0.01). Both a stress factor (mental workload, OR 3.5 (2.52 - 5.00)) and a stress buffering factor (work rewards, OR 0.3 (0.23 - 0.46)) were significantly associated with burnout.
Click to view | Table 3. Logistic Regression Analysis of Burnout and SOC Groups, Mean Working Hours, Job Stress, and Buffer Factors (n = 834) |
| Discussion | ▴Top |
In the present study, even after adjusting for stress factors and stress buffering factors, SOC score was significantly associated with burnout. Attending physicians in the low SOC group had a 4.7-fold higher risk of burnout than those in the high SOC group. In a previous study of Japanese workers, the risk ratio for job absence due to depression was 0.18 in the high SOC group when the low SOC group was used as the reference [22]. In a study of medical residents, the OR for future depression was 3.11 in the low SOC group when the high SOC group was used as the reference [20]. In the present study, the prevalence of burnout was very low (3.2%) in physicians in the high SOC group. This suggests that attending physicians with low SOC scores tend to experience burnout, as is the case in other professions and in medical residents.
Higher weekly working hours were also associated with burnout. Physicians who worked over 100 h weekly had a 7.8-fold higher risk of burnout compared with physicians who worked fewer than 60 h weekly. In a previous study, 38.5% of residents who worked fewer than 80 h weekly experienced burnout, compared to 69.2% of those who worked over 80 h weekly [10]. The Accreditation Council for Graduate Medical Education (ACGME) restricted the working hours of residents to under 80 per week in 2003 [23, 24]. Since the present study found that the negative effects of long working hours were similar in attending physicians and residents, the former might also benefit from working hour reductions.
In the present study, both a stress factor and a buffering factor were associated with burnout (adjusted ORs: mental workload, 3.5; work rewards, 0.3). In a previous study investigating the relationship between residents and depression, of the six BSJS subscales, three stress factors (workload, mental workload, problems in personal relationships) had a positive correlation with depression, while one buffering factor (reward from work) had a negative correlation [14]. In another study of residents, depression was associated with mental workload (OR 1.86), problems in personal relationships (OR 1.92), and reward from work (OR 0.59) [21]. These findings in residents were similar to those of the present study in attending physicians.
Logistic regression analysis showed that SOC was an important predictive factor for burnout after adjusting for stress factors and buffering factors. It is possible that addressing only the known contributors to burnout, namely working hours, stress factors, and buffering factors, is inadequate, and appropriate care and intervention should be provided to attending physicians who have low SOC scores. For example, short, frequent counseling sessions informing physicians with low SOC scores that they are at high risk of burnout may lead to altered behaviors and the prevention of burnout.
This study has several limitations. First, physicians already experiencing burnout might not have attended the training sessions and workshops where we recruited our study participants. Thus it is possible that we over- or underestimated the number of attending physicians with burnout. Second, only 48 (35.6%) organizers participated in this study, a relatively small percentage that might have led to sampling bias. Organizers of training sessions and workshops for attending physicians must register with the Japanese government, so it would be possible to identify all organizers across Japan and ask for their participation. However, expanding our study to include all organizers would be unlikely to substantially influence the results, as the distribution of organizer types was similar in this study and nationwide. Third, since this study used a cross-sectional design, we could not determine a causal relationship between stress factors and burnout. Thus, further research is needed to determine whether interventions for attending physicians who have low SOC scores are effective for preventing burnout.
Conclusions
In this study, burnout among attending physicians was significantly associated with SOC scores after adjustment for stress factors and buffering factors. This result may help prevent burnout among attending physicians by informing the establishment of an effective support system.
Acknowledgments
The authors wish to acknowledge all organizers of the training sessions and workshops where subjects were recruited, as well as the attending physicians who participated in this study, for their generous cooperation.
Ethics Approval
The study was approved by the Ethics Committee of the Faculty of Medicine of the University of Tsukuba, No. 774-1.
Competing Interests
The authors declare that they have no competing interests.
Funding
None.
Grant Support
There is no grant support for this study.
Author Contributions
YK contributed to the study concept and design, data acquisition, analysis and interpretation, and the drafting of the article. AT contributed to the study concept and design, data acquisition, analysis and interpretation, and the revision of the manuscript. MI contributed to data acquisition, analysis and interpretation, and the revision of the manuscript. TaM contributed to data analysis and interpretation and the revision of the manuscript. ES contributed to data interpretation and the revision of the manuscript. TeM contributed to the study concept and design and the revision of the manuscript. All authors approved the final manuscript for submission and agreed to be accountable for all aspects of the work in terms of ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
| References | ▴Top |
- Fahrenkopf AM, Sectish TC, Barger LK, Sharek PJ, Lewin D, Chiang VW, Edwards S, et al. Rates of medication errors among depressed and burnt out residents: prospective cohort study. BMJ. 2008;336(7642):488-491.
doi pubmed - Shanafelt TD, West CP, Sloan JA, Novotny PJ, Poland GA, Menaker R, Rummans TA, et al. Career fit and burnout among academic faculty. Arch Intern Med. 2009;169(10):990-995.
doi pubmed - West CP, Halvorsen AJ, Swenson SL, McDonald FS. Burnout and distress among internal medicine program directors: results of a national survey. J Gen Intern Med. 2013;28(8):1056-1063.
doi pubmed - Kitaoka K, Masuda S. Academic report on burnout among Japanese nurses. Jpn J Nurs Sci. 2013;10(2):273-279.
doi pubmed - Nishimura K, Nakamura F, Takegami M, Fukuhara S, Nakagawara J, Ogasawara K, Ono J, et al. Cross-sectional survey of workload and burnout among Japanese physicians working in stroke care: the nationwide survey of acute stroke care capacity for proper designation of comprehensive stroke center in Japan (J-ASPECT) study. Circ Cardiovasc Qual Outcomes. 2014;7(3):414-422.
doi pubmed - NIOSH working group. Stress at work; volume 8. Cincinnati: National Institute for Occupational Safety and Health (NIOSH); 1999.
- Hurrell JJ, Jr., McLaney MA. Exposure to job stress--a new psychometric instrument. Scand J Work Environ Health. 1988;14(Suppl 1):27-28.
pubmed - Shanafelt TD, Balch CM, Bechamps GJ, Russell T, Dyrbye L, Satele D, Collicott P, et al. Burnout and career satisfaction among American surgeons. Ann Surg. 2009;250(3):463-471.
doi - Jovanovic N, Podlesek A, Volpe U, Barrett E, Ferrari S, Rojnic Kuzman M, Wuyts P, et al. Burnout syndrome among psychiatric trainees in 22 countries: Risk increased by long working hours, lack of supervision, and psychiatry not being first career choice. Eur Psychiatry. 2016;32:34-41.
doi pubmed - Martini S, Arfken CL, Balon R. Comparison of burnout among medical residents before and after the implementation of work hours limits. Acad Psychiatry. 2006;30(4):352-355.
doi pubmed - Linzer M, Visser MR, Oort FJ, Smets EM, McMurray JE, de Haes HC. Predicting and preventing physician burnout: results from the United States and the Netherlands. Am J Med. 2001;111(2):170-175.
doi - Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med. 1993;36(6):725-733.
doi - Tselebis A, Moulou A, Ilias I. Burnout versus depression and sense of coherence: study of Greek nursing staff. Nurs Health Sci. 2001;3(2):69-71.
doi pubmed - Haoka T, Sasahara S, Tomotsune Y, Yoshino S, Maeno T, Matsuzaki I. The effect of stress-related factors on mental health status among resident doctors in Japan. Med Educ. 2010;44(8):826-834.
doi pubmed - Maslach C, Jackson SE, Leiter MP. Maslachburnout inventory manual. 3rd edn. Menlo Park: Mind Garden; 1996.
- Kitaoka-Higashiguchi K, Ogino K, Masuda S. [Validation of a Japanese research version of the Maslach Burnout Inventory-General Survey]. Shinrigaku Kenkyu. 2004;75(5):415-419.
doi pubmed - Togari T, Yamazaki Y. Examination of the reliability and factor validity of 13-item five-point version Sense of Coherence Scale. Jpn J Health Hum Ecology. 2005;71(4):168-182. (in Japanese).
doi - Gintare Kaliniene RU, Lina Skemiene. Assessment of work related stress among female public service workers. Central European Journal of Medicine. 2013;8(6):861-870.
doi - Nishikido N, Kageyama T, Kobayasi T, Haratani T. Assesment of job stress using a brief questionnaire: its relations to depression among male workers of an information processing company. Occup Ment Health. 2000;8(2):73-82. (in Japanese).
- Ito M, Seo E, Ogawa R, Sanuki M, Maeno T. Can we predict future depression in residents before the start of clinical training? Med Educ. 2015;49(2):215-223.
doi pubmed - Yokoya S, Seo E, Ogawa R, Takayashiki A, Maeno T. The effect of stress-related factors on depressive state among medical residents. Medical Research Archives. 2016;4(6):1-12.
doi - Sairenchi T, Haruyama Y, Ishikawa Y, Wada K, Kimura K, Muto T. Sense of coherence as a predictor of onset of depression among Japanese workers: a cohort study. BMC Public Health. 2011;11:205.
doi pubmed - The ACGME’s approach to limit resident duty hours 12 months after implementation: a summary of achievements. In: Accreditation Council for Graduate Medical Education (ACGME). Available from: http://www.acgme.org/portals/0/pfassets/publicationspapers/dh_dutyhoursummary2003-04.pdf.
- Vetto JT, Robbins D. Impact of the recent reduction in working hours (the 80 hour work week) on surgical resident cancer education. J Cancer Educ. 2005;20(1):23-27.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution Non-Commercial 4.0 International License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Clinical Medicine Research is published by Elmer Press Inc.